There was a time when I would pull the bright orange lanyard over my head with some sort of ferocity, some sort of determination. In white letters it says, “Parent/Caregiver.” I walked the halls by morning and day. In evening and night the orange encircled my neck. A color impossible to disregard. A color that declared, “In this place I dwell and in this place I fight. When you look at me, know there is a face of a small child behind a door you will likely never see. But she is there. And I am here and I will not let you forget that she is real. When you see my fatigue, know there is a child battling for her life. When you see my joy, know there is a child whose life is being saved in this building. When you see the puffiness of eye lids, a face strained from tears that both never cease to fall and never cease to be sufficient, know that a child’s life teeters on the edge and pleads for more – more days to run outside with wind on the face. This orange pleads for more – more options when it seems there are none left and more weapons with which to fight that don’t also come at the cost of intelligence, of growth, of a heart that will allow her to run, to run.
There was a time when I would pull the bright orange lanyard over my head with some sort of ferocity, some sort of determination. In white letters it says, “Parent/Caregiver.” I walked the halls by morning and day. In evening and night the orange encircled my neck. A color impossible to disregard. A color that declared, “In this place I dwell and in this place I fight. When you look at me, know there is a face of a small child behind a door you will likely never see. But she is there. And I am here and I will not let you forget that she is real. When you see my fatigue, know there is a child battling for her life. When you see my joy, know there is a child whose life is being saved in this building. When you see the puffiness of eye lids, a face strained from tears that both never cease to fall and never cease to be sufficient, know that a child’s life teeters on the edge and pleads for more – more days to run outside with wind on the face. This orange pleads for more – more options when it seems there are none left and more weapons with which to fight that don’t also come at the cost of intelligence, of growth, of a heart that will allow her to run, to run.
In more recent times I refuse to wear the orange lanyard. I comply. Its circle swings from my arm. Most often it clashes with my outfit, the one selected for its pleasing combination of colors, of texture and pattern. That orange just slices right through it, distracting, demanding attention. Rebellion. Small, almost unrecognizable, but I know, I know that I am a “Caregiver,” but this is not all that defines me. I rebel and declare that I have an existence outside of this place. This orange does define me but it takes all the focus and lest you forget, I am more than a woman hidden away in this place.
We were finally settled into our new room in the Forest PICU, the one with the familiar bed and happy little raccoon stenciled on the glass. The green of new flower bud in the hallway cheers and bursts, life, life, life! I asked the nurse if she knew what time rounds would be in the morning so I could decide when to set my alarm in order to be ready to stand in the circle with the team that each morning joins together to consider Allistaire. “You could just sleep until rounds and shower after,” she replies. “I don’t do that,” I say in short staccato. She comes back with, “You don’t have to look glamorous.” Glamor? Hah! It’s not about glamor. It’s about rebellion. It’s about defiance. It’s staking a claim and declaring that we exist outside of disease. It is a shout that though you may see a bald child with tubes hanging all off her in a disarray, though you may see BNPs, CRPs, SVO2s, BUNs, phosphorus and calcium levels, creatinine, AST and ALT, WBC and abdominal girth, hematocrit and platelets counts – they are not the sum of her! When I stand, clothed for the day, in that circle of doctors and nurses, I stand for her. I stand ready to fight another day.
In the darkened room of nap time, I sit on the side of her bed rubbing her back as she moans. Asleep but eyes squinting in pain. I run my fingers up the length of her unfathomably soft back, up the nape of her neck where a wee nest of fine blonde hairs have defended their territory, up, up over the perfect curvature of her cranium. A familiar routine, but I am startled as I look at her face. She is a girl. I take in her features and the adorable curve of her nose, the little light freckles newly scattered across the top of her cheek and realize, she is a girl. I can see it suddenly. She is no longer baby or toddler, but girl. So long she has been bald, and even now, though she is forced to wear diapers, I see her long legs stretching out across the bed. I see it in her face. She is a girl in the world. Earlier she cried out, “It’s not fair, it’s not fair.” She cried because she so desperately wants to eat, wants to drink. For the last thirteen days she has been forbid this essential human act. I don’t know where she got this language, “fair.” It is not a word I use because nothing about life is fair, not the good, not the bad. There is no earning the bountiful good I have generously been given. There is no earning this sorrow. But I saw, her not as sick child in a bed, not as that baby girl that I gave birth to, not this wee girl I have cared for so long in the hospital, but a girl, her own self.
I stroked her back. It is not only my child whose life is at stake. It is not just the dreams I have for that baby I carried in my womb. She is her own spark. Her life so overlapped with mine has its own perimeter. She is her own girl and I suddenly longed so sharply for her own self to have opportunity to force its way up into the world like that young tender stalk of flower pressing up through the dark soil, bud curved and unfurling, shining it’s own color out into the light. I stroked her back and took in the adorable curve of her nose and was startled to imagine the sight of a woman there, a woman much older, decades older, dying again of cancer, of heart failure, of kidney disease. And sudden grief overwhelmed as it came so clear that though she may live, this brutality of treatment may come snarling at her heels, threatening to ensnare such vibrant life, snap at her throat or silently constrict. Her echocardiogram on Tuesday was worse than before. Her ejection fraction dropped to 23 (previously 65 down to 29) and her shortening fraction dropped to 13 (previously 32 down to 18). I shudder at the thought of an older version of myself stroking my daughter’s forehead as she once again fights so hard for life.
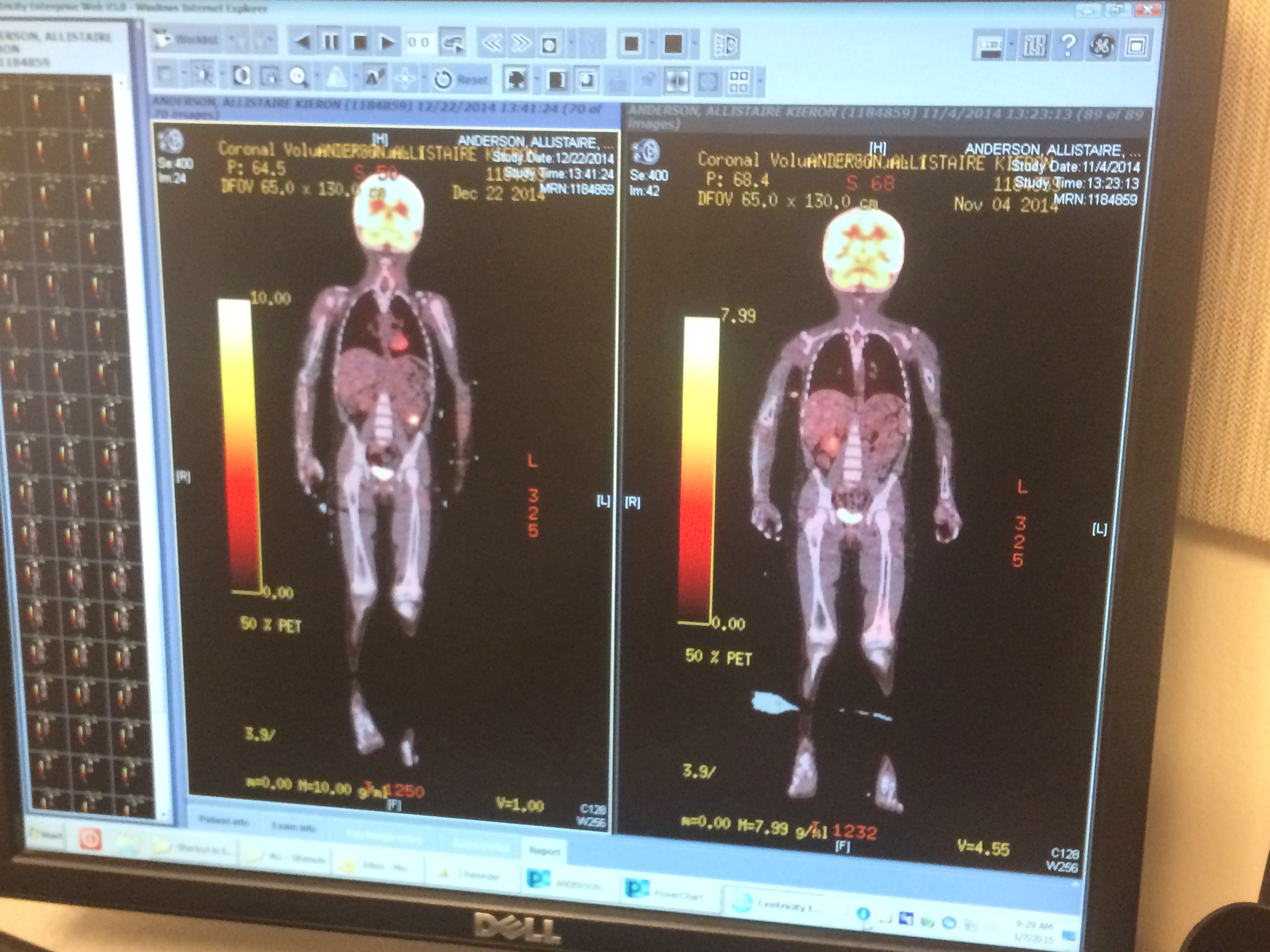
Yesterday, the foreboding CT finally came. Over the course of more than an hour, Allistaire took tiny sips of apple juice mixed with contrast in anticipation of the scan. When at last the contrast was in, the required hour had passed and the careful preparation to transport her to CT was nearly complete, Lauren, our nurse informs that we are just waiting a bit longer because the team wants to add on a few things. Add on what? “They want to look at her sinuses and brain.” My mind goes immediately to black mildew of showers, to pink mold growing in the gray curves and undulations of her brain. Fungus in the brain? Oh good grief! Another terror to top onto a great pile of terrors. And in the lull of quiet after returning from CT and getting her all settled in, I tried to pray, knowing results would not take too long.
In little bursts I began to pray. My words stepped out this way and that but each time retracted. What do I pray? What can I possibly say to the Lord that hasn’t been said already a hundred thousand times? Of course He knows I long to have Allistaire be well and all the results be good. He knows that. I don’t even need to speak the words for Him to know my longing for her. But I cannot ask for anything less than good, I cannot ask for there to be fungus lurking in the crevasses of her flesh. Fungus is hard to treat. Fungus takes a long time to treat. Fungus can actually be the death of you. My whole being strains forward in anticipation of the day when all this is behind us, when we have not only come to transplant but when we can look at it stretching out behind us like far off mountains, and we turn with eager joy as we speed East on I90. While we remain trapped in this endless cycle of fighting cancer, my heart soars beyond it, out to the meadow in front of our house where crickets sing in evening and sage swells in the coolness, where grasses of innumerable sorts, grasses of blue and pink, brown, green and black undulate in waves of wind. Like Dorothy, I long to return home, to the simple perfect joy of making dinner and looking out the window occasionally, seeing Solveig and Allistaire making their fort in the bushes along the driveway.
I willfully shift my gaze from that scene, I fix my eyes on Christ. How many times have I handed her over to Him? How many times have I asked Him to help me yield to His vision. What can I pray? She is yours Lord. All her days are yours and I must even let go of telling Him how it is okay for her to die. Somehow I have unconsciously decided that if she must die, let it be when all else has failed, let it be when she has exhausted every opportunity to fight. To die of fungus? To die when the road to transplant is laid open before us? No! NO! Such indignity to die of fungus, to die of a heart that just finally fizzles out. But who am I to say? This fight against cancer demands all the attention, but really, cancer is not the point. Sickness and disease is not what this is about.
I reorient my heart to Him. I yield and allow the tug on my heart to pull me in, to draw near to Him. To look Him in the eye and say, Yes. Whatever you will Lord, whatever You will because your view of this landscape is not just of mountains, sorrow looming on the horizon behind and before. You see the mountains, every crag and riven rock. You were there when the plates of the earth contorted and bent in waves of rock. You see the mountain goat windswept. You see the blue-gray ferocity of storm and bright liquid yellow breaking through. You are acquainted thoroughly with wee bug on leaf blade, of bacteria eating away the decay of leaves producing beautifully complex antibiotics to secure their survival against competitors. You Lord are not bound by time, by place, by great expanses of space or the infinitesimally small distances between nucleic acids woven together in double helix. You are the God whose eyes pierce my heart and discern every nuance. You are the God who has come down low and looks each of us in the eye, with compassion and love swelling.
This is not about whether or not there is fungus in her brain that brings death. This is not about Typhlitis or leukemia. This is not about whether she lives to her 5th birthday, 35th or 80th. This whole thing, every last detail is all about a beautiful God to wrestle with, to call upon, to yield to and know true abundant, eternal life. This life, right here, this life is, according to Him, a vapor, a passing mist. The mystery though, the elegant paradox, is not that this temporal life doesn’t matter or is insignificant, rather it is through this passing life that we may come to possess, through Christ, life that never fades, never fails, never diminishes. We are blessed in this passing life to both come to know the Living God who matters ultimately and to know that these troubles will pass away, they will not forever bind us. What mysterious gift to be able to deeply and vastly treasure this present life and to simultaneously hope for eternal life where every tear is wiped away, where sin and death have been forever conquered and where we will delight to see our Lord no longer through veil. What freedom to hold what is precious with open palm.
This is the paradox I hold each time I come to the Lord in prayer. Oh how I love and treasure the life of my child and the delight I gain in knowing her. I want my sweet young girl to have the chance to experience this life. So of course He knows I long for her to be healed. And honestly, that is an easy prayer. Effortlessly, I ask for good test results, for long life for Allistaire. Wrestling fills the bulk of my prayers. Lord, help me to love others enough to endure suffering for their good. I cringe at the thought of likening myself to Christ for I fail so overwhelmedly, but He has set it in my heart to see that as I lay down my life in submission to His will, He uses the tears of my sorrows to raise up life. For it is so intensely in these crushing crucibles of suffering that His face and voice have become most clear. It is in these small cramped spaces of isolation and constriction and loss that I actually gain Him. His words, which I have long believed, have become known, affirmed and beloved in ways I had never known prior to these last four years. I have come to possess the Living God as He has drawn me in to greater dependence on Him. He is my treasure. How wild that I should gain the Ancient of Days?! Who am I to have been given entrance to His heart, to His pounding, faithful love? But it is precisely here, right here, in all the black moments and seasons that I have most seen His light. Who am I to say No to that? How can I say I don’t want to see Him? How small would my love be for my dear fellow creatures if I did not yearn for each to know such deep, pervasive, uncollapsable joy?
Lord you know my heart. Your will be done. More and more I am able to yield. Brain fungus? I want to shout and stomp a furious, “NO!” But I am the small one, the one with limited sight. Be Thou my vision, oh Lord of my heart.
As it turns out, the resident comes in gleaming. It’s all good. No brain fungus. No fungus or scary unexpected infections anywhere and a gut that is clearly on the mend. And I praise the Lord. Thank you Father. Thank you for this good gift. Wahoooo! Rejoice, rejoice, rejoice! As I nearly ran into the hospital this morning after going over to Ron Don to pack my clothes for the next several days, I heard singing! Birds, birds, singing, singing. Oh wonder of spring that defies the cold, defies the dead of winter. There are cherry blossoms that as always, decide so seemingly early, they are done with the drear. They shower the tree boughs with cheery pinks. The rock daphnes perfume the air. There are yellow crocuses bursting out of the ground in front of the Ronald McDonald House sign. Strange pale green, cabbage-like leaves are unfurling. We know in our gut that life ought prevail. And so it does, sometimes in this present life and always, always in the life to come.