
 The dark grey blue of cloud bellies move slowly east, sheets of rain stretching out, connecting sky to earth. Thunder lumbers and bellows. Rain hits hard on the roof. A flash of lightning. Quiet. The storm moves on and the sky opens to blue. To the west, to the south, the sun glints on the Spanish Peaks illuminating their vertical striations of rock and ridge, Beehive bright tucked behind. Then shrouding of white, thin wisps of rain stranding from grey to light in the evening sun.
The dark grey blue of cloud bellies move slowly east, sheets of rain stretching out, connecting sky to earth. Thunder lumbers and bellows. Rain hits hard on the roof. A flash of lightning. Quiet. The storm moves on and the sky opens to blue. To the west, to the south, the sun glints on the Spanish Peaks illuminating their vertical striations of rock and ridge, Beehive bright tucked behind. Then shrouding of white, thin wisps of rain stranding from grey to light in the evening sun.
More thunder, cracks of power break open overhead, the darkness of more clouds heading this way.
“I don’t know how to do this,” I say to Dr. Cooper with a restrained wail in my voice, “I guess you have to just live each minute.” There is always the before and after, a thousand points marked off, striating, separating then and now, what was, what is. Eventually the “what will be,” becomes the “is.” A hundred thousand test results, countless days and hours and minutes for the heart to beat hard with suffocating thud, anticipating the blade coming against your throat. The wave rips you off your feet, dark weight pressing down on you, flailing, desperation to right yourself. Gasp of air and crashing wave grinding you down again and again.
Quiet. Eery, odd, quiet. Calm. Flat face. So this is how this goes. This is how minutes amass to hours and days, months into years. So this is how death comes. This is how the thievery of your child’s bursting life gets stripped away, paint ripping in shreds from boards exposed too long in harsh weather, the slow erosion of flesh, the silent march of invasion.
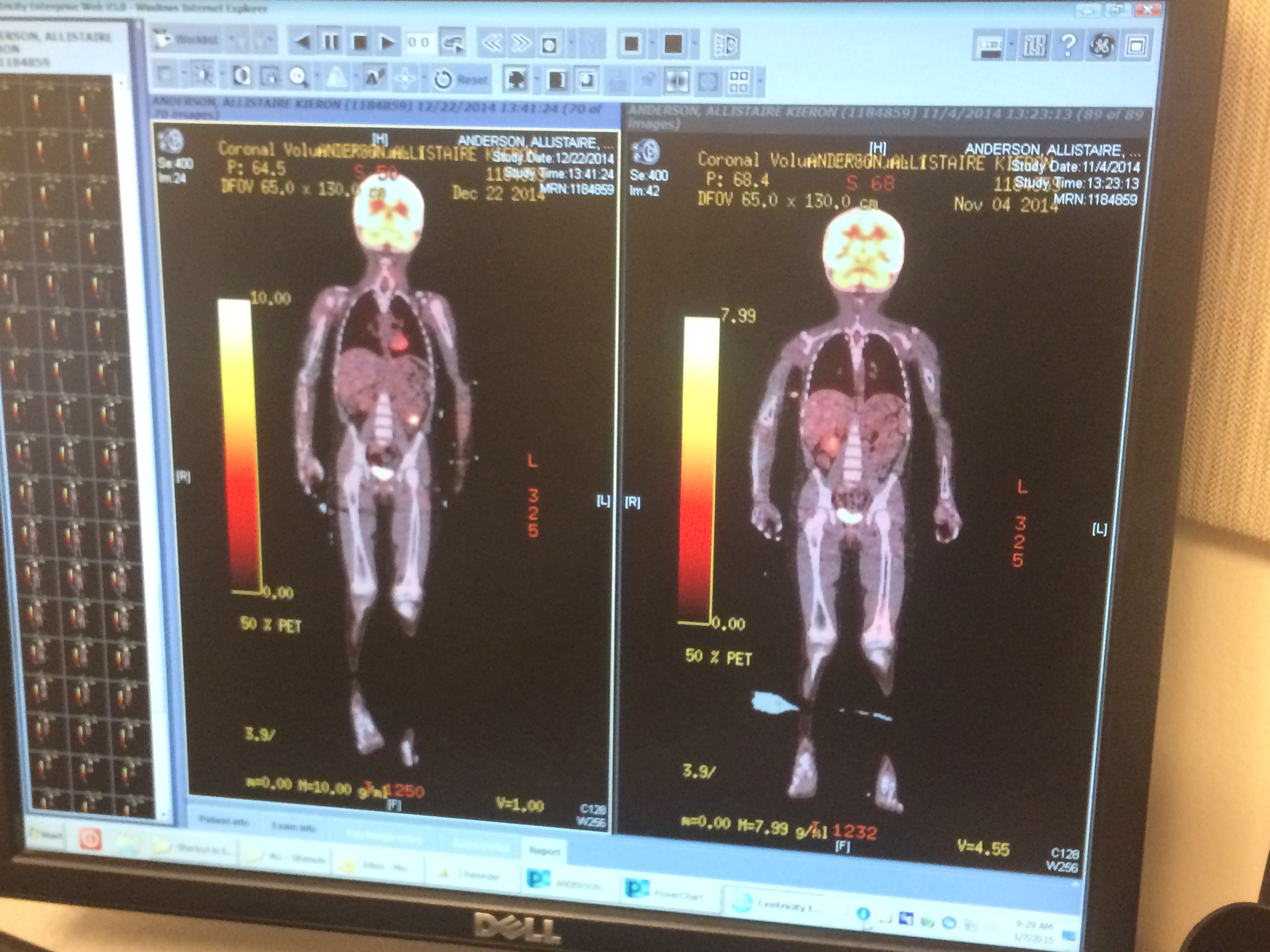
Dr. Eagan, the PI (principal investigator) of the WT1 T-cell trial said Allistaire’s chloromas just amounted to too much disease to have hope that the T-cells would be successful, at least at this point. In addition to the 6-7 chloromas in her spine, sternum and pelvis seen on the last PET/CT, four out of two hundred cells tested from her bone marrow aspirate showed Allistaire’s MLL (Multi Lineage Leukemia) mutation according to FISH (Fluorescence in situ hybridization). The Flow Cytometry test showed 0% detectable leukemia in her marrow. There was not even enough disease in the chloromas for corresponding masses to show up on CT. Only about 5 years ago there would have been no detectable disease anywhere – there was no Flow Cytometry and PET scans weren’t used for leukemia. Even a year ago Allistaire had never had a PET scan, only CTs to look for chloromas. We would all think she was cancer free, in remission. That was then, this is now.
Since we couldn’t move forward with the T-cells with any hope of success, the goal is to see if we can get her in a better spot. Her heart is still far too weak to endure any intense chemo. The accumulation of hard chemo has killed muscle cells in her heart that will never be replaced. They are dead. There is nothing new to replace them, only the hope that the surrounding cells can compensate for their loss. The very weapon wielded against her cancer has cut her through, has permanently wounded her. This is why there is no transplant on the horizon. It is for now, off the table. There is no plan to move forward with a transplant.
So Dr. Cooper, after much thought and consideration recommended the course of treatment that we have chosen to pursue. She began five days of Decitabine last Friday which will be followed with three doses of Mylotarg (generic name: Gemtuzumab) on days 6, 9 and 12 of this round. Gemtuzumab is an antibody which is bound to the chemo molecule, ozogamicin, which then binds to the CD33 antigen receptor on the cell surface of myeloid cells (which is the cell line that is cancerous in Acute Myeloid Leukemia). Once the Gemtuzumab antibody binds to the CD33 antigen, the whole molecular complex moves inside the cell where the cytotoxic molecule, ozogamicin, kills the cell. “Calicheamicins (of which Ozogamicin is a derivative) target DNA and cause strand scission. Calicheamicins bind with DNA in the minor groove, wherein they then undergo a reaction analogous to the Bergman cyclization to generate a diradical species. This diradical, 1,4-didehydrobenzene, then abstracts hydrogen atoms from the deoxyribose (sugar) backbone of DNA, which ultimately leads to strand scission.[6] The specificity of binding of calicheamicin to the minor groove of DNA was demonstrated by Crothers et al. (1999) to be due to the aryltetrasaccharide group of the molecule.” I included that last bit from Wikepedia because I love the wild intricacies of our flesh. And because I’m sick and tired of people offering me simplified cures for cancer. Essential oils do not cure cancer. Juicing doesn’t cure cancer. Cancer is a beast of a million, trillion heads with thousands of faces ever-changing, mutating, hiding and lunging out again to strangle the life out of you.
If you read about Gemtuzumab, you will see it has a dark past and was pulled by the FDA in 2010. Allistaire is actually only able to get it on a compassionate use basis. However, questions about the trial that caused alarm over its perceived toxicity and lack of efficacy, have shown that it may not have been the right move to pull it. It has remained available in Europe and more recent trials have shown promise. Allistaire will receive her first dose this Wednesday. The primary concerns are immediate allergic responses like anaphylactic shock which she will be pre-meded with Benadryl and longer term concerns for her liver including VOD (Veno Occlusive Disease).
….That was Monday, today is Saturday. In the week preceding Monday, Allistaire, Solveig, Sten and I drove east on I90 all the way home to Bozeman. Dr. Cooper supported us going home for a visit – Allistaire’s first time home since she left in October. Sten took the girls to clinic on Wednesday morning, July 1st so I could pack without them knowing in case labs were bad and we’d be thwarted at the last moment. But labs were fabulous and when the girls opened the door, Allistaire asked why all the bags were packed on the floor. “We’re going home to Montana for a visit, sweet girl.” She was beside herself. She couldn’t articulate her amazement and joy. I’d say she was flabbergasted and it was the best. I loved that joy. After staying the night in Spokane as we have done so many, many times we continued on east through a land that all cells of my skin, eyes, hair, fingernails all sought to soak in, like dear friends with whom you have long yearned to visit – blue of Lake Coeur D’Alene, marshy grasslands before Cataldo in Idaho, my great big hill I plan to climb one day – a hill already turning yellow in summer’s heat but great and white in winter’s cloak and shocking purple in spring with billions of flowers of a name I don’t know, that curve of rock that repeats pinks and purples of setting suns, a great boulder over green water – a swimming hole I imagine diving into its cool deeps and drying out in the warmth of the rock, tumbling great rounded groupings of rock like a Flintstone landscape over Homestake Pass, the river bottom with Cottonwoods in Whitehall and up that great curve of road that will soon bring my eyes to rest on the Bridgers in the distance – the mountains that are mouth to my home, to Kelly Canyon with its aspens, Rocky Creek, Bridger Creek, magpies and coyotes, black bears and deer, scores of red-winged black birds calling their eery beautiful cry in morning and evening, pairs of sand-hill cranes who sound as if they have mistaken Montana for Africa. There a multitude of colors of grass like waves moving in the wind over the contours of the land, punctuated by the silvery blue of sagebrush, that wondrous smell of moist coolness of night soaked up in their leaves and released like blessing. At long last we were home, home.
Every joy paired with splitting pain. The familiar strange smell of our house built in the 70’s. Waking to light on the Spanish Peaks, light on leaves and flowers and the great evergreens on the hill, piercing blue of summer sky. The feel of smooth tile underfoot as I stumble to my bathroom at night – no handicap bar just lush toilet paper. Spying Allistaire sitting on her closet floor playing with her toys in the morning, her sweet blonde head ascending the stairs to greet the day. Birdnest ferns and mother ferns, variegated leaves and leaves pink, leaves with purple, plump sculptural succulents and fuchsia of orchid petals, light broken in pieces of rainbow color by the prisms in the windows, the delectable breeze moving up the canyon and occasional ring of wind chimes. Sitting down together for pancakes, four in a row along the kitchen counter. Sending laundry down the shoot, into the wash and taking it out to the line to dry in the already hot day. When I went into the garage I broke down. Fishing poles and life jackets and bikes and buckets and pairs of little shovels and bug catchers and gardening gloves with childish patterns, hiking boots and a bike rack – a life once lived. A life stalled. A life paused. A life cut short? I think of going to Cliff Lake last year and my heart breaks open. How desperate I am for the smell of campfire and the negotiation of how many marshmallows are reasonable. I pant for Hyalite, for the simple extravagant pleasure of driving up that road and seeing water ringed by mountains, of packing coolers for picnics and the heft of a pack on my back as we ascend through the forest. I watch the girls out the kitchen window, they head to the thicket of bushes where they made a fort last summer, the little blue bucket having finally been removed from the branch where it hung for months. They play long with a caterpillar, lovingly making it a home to enjoy and hit jackpot when I find what I told them was a baby mouse, but I now think must have been a vole. They carry it back and forth with gloved hands, tender in their care and wonder.
We had a wonderful week all together and time with family. On her last evening home, we celebrated sweet Per’s third birthday. Allistaire rode the tricycle in her yellow dress with great blooms – a french girl’s dress. Up and down the sidewalk she went. At last it was time to say goodnight, but not just goodnight, goodbye. And I watched as simple hugs and goodbye’s were exchanged and suppressed the desire to cry out, to yell – “do you not realize you may never see her here again?” Every joy sat side by side with the fear that these days would never be again, that I was witness to the lasts of many things, things simple, things mightily beautiful, treasured beyond all else I possess. Next to the image of her yellow dress and happy face in the waning light sat deep sadness that she was alone, no one to play with, a child who has so seldomly been able to play with her peers, with really any children at all. The older two, Solveig and Haaken, were off on their big kid adventures and Per was enamored with the little neighbor girl. Next to the image of her that night, an image of seeming lighthearted joy, sat images of Carly’s face with tumors bulging, pressing tight and purple and shiny taut against the skin, eye distorted. I saw Benton’s face deformed by numerous tumors that contorted his features. I saw his face laying in a casket as I filed past, tears streaming. I knew I had seen something that terrified me. Something I wanted to ignore, to disregard, to cover with more plausible explanation, but I turned back to it over and over and over, examining, questioning – what do I see there? Something seems off. Her right eye, something is not right, something is not normal. What is it? What am I seeing?
Sten drove her back to Seattle on Thursday so she could begin chemo on Friday. He came to Allistaire’s appointment with Dr. Cooper with a list of questions I had, questions with answers relayed and more questions lobbied back. Nestled in amongst the questions of did we really know if Allistaire’s cancer expressed CD33 and how do you know how many days and on what days to give Mylotarg, was the question, do you see something off with her right eye? Yes, ptosis, a droopy or falling eyelid, an effect on the muscles of the eye. Sten’s voice on the phone, “He ordered an MRI.” “Oh God, why? What is he thinking it might be?” Later Dr. Cooper and I talk on the phone and he was concerned. It could be a tumor pressing on nerves in her spine or in her brain.
For days Solveig and I were alone. Just the two of us. Just like old times. Times when she was my little buddy and we went everywhere, just the two of us. How dear she was to me, how overlapped with my life. Then I had a miscarriage, a DNC, months of trying to get pregnant again, fear of miscarriage all over again. Sorrow, fear, acrid poisons seeping into the crevasses of my heart and mind, weighing down my finger tips and shoulders. Sober. A turning. I couldn’t laugh as easily. Other private wounds and weeping added one to the other, layers pressing down. Desperate cries to the Lord, a turning to the Lord like never before. My first tastes of Christ as my very life, Christ the very fuel of my cells, the brightness of my eyes, my longing, my aching need for Him and the sweet, sweet knowing of really tasting the beauty of the Lord. Sober. Deep expanses opening up, being broken open down into the very core of myself. A fundamental tearing, sinews strained and snapping, bleeding out, faint. In these four plus broken years I’ve felt too weak to love Solveig as she deserves, as I long to love her and gosh, oh man do I love that girl. I hunger for her eyes, her giddy laugh, her brown ringlets she desperately wants straight, her skinned bruised legs from play, the magnetic irresistible draw of books, of stories for her budding mind, her unstoppable creativity, the ever request for a back rub. I love Solveig Kailen Anderson and I have missed that girl. I have missed so much of her life because of all this with Allistaire. When she was only as old as Allistaire is now, we sent her to Montana to live with her grandparents while I fought alongside Allistaire in the hospital. The first relapse meant 8 months away from home and four plus more months of constant week-long trips back to Seattle. This relapse it’s already been 9 months with no end but the worst in sight.
For three weeks I had the joy of being with Solveig, the most time I’ve spent with her in all these nine long months. When at last Monday came and loomed as the day I would lay down to sleep knowing something more, something of that eye, I talked with Solveig. I attempted to prepare her for what may be coming. Dr. Cooper called around 5:30pm. It’s not in her brain, but there is a 2 1/2 cm mass of leukemia in her right sinus. It has begun to erode away the bone. The tumor, the chloroma, is putting pressure on the muscles which operate her right eye, that’s why it doesn’t look right. Right there. Right there smack in the middle of my little sweet girl’s face dwells an insidious tumor that threatens to take more, to distort, to ravage, to gnaw. There is also a very small one in her left sinus. Dr. Cooper knows of children in which the leukemia eats away the bone into the brain. Why Lord? Oh God please, please don’t take her this way.
With shoulders slumped I came to face Solveig, to tell her this latest revelation of the onslaught of Allistaire’s disease. I asked her, gently pleaded, be kind to your sister. You don’t know how many days you may have with her. Don’t fight over toys. Treasure her, for one day we may have no medicine left to stop her cancer. One day we may need to bring her home to this house to lovingly surround her as she dies. I tell Solveig that she will not be the same girl she once was. She may not be able to walk. Her face may be distorted with tumors. Her eyes may not work. Will she be able to speak? The imaginings are so brutal. It just ravages my heart to imagine this for her. Oh God it hurts, it hurts so bad. Solveig is silent and then sobs heave and tears stream. I hold her close and grieve time lost and a possible future without her sister. How I so loved the thought of two sisters growing up together. Solveig by herself, just another sorrow, another gaping wound.
The thing is, I can see on the other side of these brutalities. I can imagine a life filled with joy. I can imagine being close to Solveig, years ahead together. I believe that there would be a day far off in the future where losing Allistaire wouldn’t decimate every day. But to get there, to walk the possible road ahead, oh how overwhelming, how utterly horrid. It is like facing the blackest tunnel, believing that it will eventually open up to light, but Oh God, how far, how long? You think, I can’t do that Lord, I just can’t bear the loss of my sweet little girl – you think this is some sort of barrier to it actually happening. I look at her little face, with that one eye askew, having many, many times a day to face that beast that is taking her. I love her. My whole flesh cries out – I love her TOO much!! I just can’t lose her. But neither is my love sufficient to hold her.
For twelve days, I soaked up Montana. I brought my bike and at long last made friends with it. I actually now crave being able to get on that seat, feet clipping easily into the pedals and heading out onto the curves of my dear Kelly Canyon. I imagine the many adventures that bike opens up to me. Morning after morning I went out into the land with vast expanse of sky opening up overhead. Glory. Absolute resplendent beauty. My sweet mother-in-law, JoMarie, so generously gave me her bike, an orange bike, a bike built for Obliteride, a bike to carry my flesh into God’s wondrous creation and a means to raise money to heal the sick. I had a fitting done at Bangtail Bikes in Bozeman and then it really became mine – it is now aligned to my body, to my outward self, propelled by the inner. Then Wednesday morning, as the first light shone blue behind the Bridgers, Sten took me to the airport. We embraced hoping not to see each other before planned in August, desperately hoping some new horror would not rise up in the next few weeks. Back to the battlefield, back to a strange life of seeming ease where I regularly drink Starbucks and sit around, but just below the surface, if you have eyes to see, is an effort of epic proportions, an unyielding fight, a straining, a grasping for life.
I returned to Seattle on Wednesday morning because Allistaire had an echocardiogram and cardiology appointment scheduled in addition to her first dose of Mylotarg. I went straight from the airport to Ron Don to drop off my suitcase and then walked as fast as I could to the hospital to make it in time for Allistaire’s labs. How strange to wake in my bed in Montana and so suddenly and utterly cast into a different world. The best news of the day was that Allistaire’s heart has gotten a wee bit stronger! Her ejection fraction rose from 29 to 36 and her shortening fraction from 16 to 21! It felt like finally being able to breathe a bit. But blast, just as we’re making some progress with her heart, her cancer is on a rampage, spreading in terrible places with still not much to combat it. Later in clinic she received Tylenol and Benadryl as pre-meds for the Mylotarg. Allistaire promptly fell asleep for the next four hours while I finally had a bit a lovely down time. Thankfully she had no reaction to the infusion and all seemed well.
After ten hours at the hospital, we finally made it back to Ron Don and I was straight worn out, having gotten up at 2:30am Washington time. Having slept so long, Allistaire completely missed lunch and now I had only a short bit of time to get dinner and meds in her. On top of it, about 8:30 that night, I noticed she felt hot and the thermometer read 102.6. Well, they were expecting this right? This is why I was given a third dose of Tylenol to give her as instructed at 9:30pm. The truth was I was wiped out and dreaded the fiasco of having to call the Hem/Onc Fellow to report the fever which I knew would result in being sent to the emergency room for blood cultures and possibly admission and antibiotics. Dr. Tarlock had warned me on Tuesday night that she may need to be admitted on Wednesday since her phosphorous and potassium were rising, signs of tumor lysis. She may need to be monitored, but her labs had improved on her own and we had skated by. But not calling in about the fever was a major failing on my part, really a huge mistake for any parent of a child with cancer. We finally went to sleep after she threw up a wretched medicine twice – a medicine meant to bind with potassium. I already had a laundry bin full when she had diarrhea twice as well and I had to change the sheets. In between all the wakings that night, I continually took her temperature and watched it steadily descend to normal. It was just because of the Mylotarg I told myself.
We were back to the hospital Thursday morning at 8am for electrolyte labs. So here’s the deal, when chemo destroys cancer cells, the cancer cells lys – they die and break open spilling all their guts into the blood stream. This is tumor lysis and it is detected by rising levels of potassium, phosphorous and uric acid. It becomes dangerous when these electrolyte levels rise steeply, beyond the limits of what the kidneys can process. Then you see the creatinine and BUN (Blood Urea Nitrogen) levels rise which indicate injury to the kidneys and the potential for kidney failure. High levels of potassium can also cause arrhythmias of the heart. So when Allistaire’s labs results returned this past Thursday morning, it was game on time. Dr. Tarlock and Dr. Cooper were amazed to see overwhelming evidence of tumor lysis with all levels skyrocketing. We were going to be admitted. Then the plan intensified with measures being taken to have an Interventional Radiology surgeon install a second central line into Allistaire with the aid of Cardiac Anesthesia for the purpose of her beginning short-term dialysis immediately. The goal was to respond quickly to this acute kidney damage and prevent kidney failure or long-term kidney damage by taking all of the burden off of the kidneys. Because of Allistaire’s heart failure, her heart would not be able to endure the huge amounts of fluid that would be necessary to help the kidney’s flush out these electrolytes. And because the kidney’s were already hurt, they could not endure the assistance of Lasix to remove the fluid. So really, dialysis was the best option. By 3pm we were once again in the ICU, this time in Forest level 5 room 321, exactly one floor down from where we spent 80 days in the ICU before.
In the time we waited for everything to be arranged, Dr. Tarlock consulted with cardiology about how much fluid Allistaire could handle on her own and she began receiving just 60ml an hour of saline. To lower Uric acid levels, she was given a dose of IV Rasburicase. She was also given Sevelamer to bind with phosphorous. The problem is, Sevelamer can only bind with phosphorous in the gut, not in the blood stream. Because Allistaire’s phosphorous was so high, Dr. Tarlock feared this would not be enough and we would need the aid of dialysis. At last we were settled in our room in the ICU. Yet when the labs drawn at 2pm came back, everything was trending in a much more positive direction due to the interventions already taken. About ten minutes into a fascinating conversation with the Interventional Radiologist about collateral veins that a young body like Allistaire’s form when other veins are damaged, the ICU attending came in to say we were going to hold off on dialysis for now and continue to monitor labs. It ended up being a crazy short and remarkably easy ICU stay. Basically Allistaire just watched movies, got her meds and some IV fluids while I tried to get food in her and grumbled that I couldn’t eat in the room. Because Allistaire was scheduled to get her second dose of Mylotarg on Saturday, we were just going to stay inpatient through Sunday with frequent labs to quickly deal with any issues if they should arise. Friday morning we were to transition upstairs to the Cancer Unit except that they had no rooms available. Finally on Saturday afternoon, we moved upstairs to the Cancer Unit into the radiation room – a room specially designed to give MIBG radiation to neuroblastoma patients. It is a lead-lined room with most surfaces being stainless steel. It’s not the most cozy room and the bed is about a foot to short due to having to accommodate the thicker lead walls. But it meant getting the show on the road and I didn’t care. I just wanted to get the Mylotarg in and get out of the hospital. At long last, on Sunday afternoon we burst out of the hospital into the blaze of a 95 degree day, having completed the second dose of Mylotarg with absolutely no issues, no fevers and labs still looking great.
Yesterday, it was back to the hospital for labs and possible platelets. I was pretty sure Allistaire would need them because of the small purple pricks of petechiae (tiny broken blood vessels) mixed in like a new wave of freckles on Allistaire’s cheeks. A single round purple bruise adorned Allistaire’s forehead right between the eyebrows like some new-age tilak mark, in this case having bonked her head on the bar of the Target cart which she was eagerly driving when it rammed a shelf. Sure enough, her platelets were 5 and so we spent the morning at the hospital getting her all tanked up. Today we head back into the hospital again for labs and her third and final dose of Mylotarg. Tomorrow, yet again, for the twelfth day in a row, we will be in the hospital for her clinic appointment with Dr. Cooper. From there…well, we wait for her marrow to eventually recover, hope no infections get her and eventually plan to do another bone marrow biopsy and PET/CT to see how things worked. After that? Who knows. If she were miraculously clear of cancer, we might be able to proceed with the infusion of modified T-cells (this is not a transplant). If she has a partial response to the Mylotarg, it may make sense to try another round of it. If there is no response or her disease has progressed, well, it all depends…of course we would investigate all our options for other treatment or the woeful possibility of being done.
Honestly, the next several weeks terrify me. Obliteride is coming up – only 17 more days. I wonder what life will look like as I ride that day. By the way, I reduced my route to the 25 mile because I just haven’t had the time to train as needed to make the 50 mile enjoyable. Three years ago on the afternoon before Obliteride, I was told that because Allistaire had disease after transplant, that she had a mere 5% chance at survival and probably wouldn’t even live 6 months. I was decimated, inside and out, that day as I rode on my old mountain bike. Last year, I physically had a hard ride, not being prepared for the 50 mile, but was propelled with determination to finish in light of all the pain and hardship Allistaire had endured. But I rode that day with hope – having had Allistaire declared cancer-free only two months prior. This year, who knows. These are very scary times. The Obliteride folks had invited Allistaire to be part of the Friday night kick-off party, but as her disease has progressed, I’ve had to say no to this, not knowing where things will stand on August 7th.
A little girl, Melissa, that I knew through friends, died of AML a week ago. Last night, my friend Kiesha and I talked as she got back labs in Missoula. It looks like Stevie has once again relapsed with AML and they will head back to St. Jude’s today or tomorrow. As I was praying for her yesterday, knowing she was trying to get labs because of all of Stevie’s bruises, I put myself back in that place of waiting for news of possible relapse. You have at long last returned to the magnificence of a “normal” life. You gaze at your child in a way that no parent of a healthy child can fully imagine – your whole self rejoices at the smallest normalcies, ordinary becomes spectacular pleasure. But when signs creep in that something is awry, the stinging is fierce and unrelenting. It is like watching a black storm on the horizon, you see it coming and you know it is about to engulf your life and twist and spin and splinter you and your beloveds until at long last you are spit out on the ground, broken, with the life pummeled out of you. It is a tsunami that sweeps you away from your life in an instant and you are put back in that place of fighting every day for life. To just simply live is all you want.
I long for a better way. I long for a day when cancer isn’t a ravager, a likely sentence of death. I long, oh I ache, for a day when the way you fight cancer doesn’t cost so much life and destruction of beautiful body parts like ovaries, and hearts and brains. I see my child. I see the children of my friends. A few have been released back into glorious life, but many stumble around from the horrific effects of radiation to the brain, limbs cut off, hearts faint, and some in caskets. Cancer is the number one killer of children by disease! I have asked many times, and I will ask again. There are so many, many worthy places to invest your resources, your money. But I am asking if you would consider giving it to further cancer research? One in two men and one in three women will get cancer in their lifetimes. You may be the one desperate for a better way, and if not you, it is almost certain that someone dear and close to you will be aching for a better way to eradicate, obliterate, cancer from their life. Cancer is personal, it comes in close to each of us. Will you join us in putting our resources to stopping this foe? One hundred percent of all the money given to Obliteride directly funds cancer research at Fred Hutchinson Cancer Research Center. Do you live in Bozeman? Do you know that the Cancer Center at the hospital is part of the SCCA – the Seattle Cancer Care Alliance which is a collaboration of Fred Hutch, the University of Washington and Seattle Children’s? Giving to Obliteride directly opens doors for clinical trials that you in Bozeman may need!
Thank you SO much to the over one hundred different people/couples/groups that have already given to further cancer research in my name through Obliteride! Yesterday, you helped me surpass my goal of $15,000. But I know there are many of you still who profess your love for us, your desire to support us in any way, who have not yet given. Would you consider honoring Allistaire’s fight in this way?
Click HERE to donate to Obliteride and directly speed up cancer research!
The research is taunting. It is moving at such an amazing pace, but I often fear Allistaire will just barely miss the thing that would at long last put down this beast of cancer. You don’t want to hear it. You think I’m crying wolf. And oh how I long for you to be right. I long for the Lord to once again make a way through for Allistaire. I know, I absolutely know He is able to heal her. I listened to the Nigerian woman tell me to pray, to fast, to believe, to test the Lord and demand He heal her as she has done for her son who is getting a transplant for Sickle Cell. She proclaimed her faith in the Lord’s ability to heal, over and over and over. But that seems too simple to me. I just don’t believe in some magic equation where enough people pray or my faith is somehow the right degree of strong and then out pops what I want. God is too big for that. He is too vast and complex and when it comes down to it – He is just OTHER than me. He is utterly “other’ and His ways are not my ways. I don’t begin to know how my little life and my little child are woven into His great plans. But the thing is, I do, I do believe they are part of the bigger picture. I don’t believe our “littleness” equals lack of significance. And what is the purpose of my life, of Allistaire’s? Is it not our great joy, fraught through with pain, to direct attention, to illuminate more the beauty of the Lord? God does not need more glory. He is not some pathetic being needing me to build Him up. No, WE need to see the glory of the Lord! We humans need to see Him for who He is that WE MAY LIVE! That is why I yield my life to the glory of the Lord – because I love, because I know my own great need to be engrafted into His life blood, that I MAY LIVE! And not just live, but live an abundant, eternal life. And in turn, I am honored that my life may in some small way direct attention to the radiance of Christ as the only source of life! May I be so audacious as to link my life to Christ’s? Is this not exactly what Christ did on an epic scale? He suffered and He laid down His life that life might spring up from His death! This is the “otherness” of God! Out of Christ’s death, the ground soaked by His blood, God overcame sin and death! He resurrected the life of Christ and in so doing made the way for redemption! Is there anything more wondrous, more mind-blowing, more exploding with glorious beauty than this? THIS is what I am invited into! In my own power, this awful road with Allistaire is just suffering, is just agony, is just death. But God is at work! He is alive and HE will take this heart of mine bleeding out as He may not remove this cup from me and He will accomplish life!
I lift my eyes to these wonders. Sometimes I am too frail and weak to even open my eyes and I need the Lord to come down low and tenderly care for me. I went to church with Jo in Bozeman and heard God’s word preached for the first time in a long time. I was reminded of God’s otherness. I was reminded of the way He blasts my rational understanding to pieces and shows me a better way, the way of life. I could hardly sing the worship songs. I just cried. I cried because the last time I was in that place was to honor Jens’ life and to mourn his death. I cried looking at the man playing the drums, wishing so desperately it could still be Jens. I cried because the words of those songs were just too much. “There may be pain in the night, but joy comes in the morning.” Oh Father, oh Father, how long is this night? The joy seems ever so far off – is there even a glimmer of light on the horizon? Words about how our life is not our own, how we give it to the Lord. That sounds nice. You can agree to that right? Your life is the Lord’s. How lovely. You sing it out with beautiful voice. Sobs fill my throat. Oh God, oh God, I do yield, I do lay down at your feet, but it is agony, it is ravaging, it feels like brutality. I cry out with Christ. My God, my God, why have you forsaken me? But I am given light on the horizon, the smallest hint of turning, I am given hope that this night will end. I read in God’s word beyond that black moment on the cross. I read of resurrection, of redemption, of light unyielding. I stake my life in the hope of God’s promises. I have tasted of the Lord and I will not turn back.
Where shall I go from your Spirit?
Or where shall I flee from your presence?
If I ascend to heaven, you are there!
If I make my bed in Sheol, you are there!
If I take the wings of the morning
and dwell in the uttermost parts of the sea,
even there your hand shall lead me,
and your right hand shall hold me.
If I say, “Surely the darkness shall cover me,
and the light about me be night,”
even the darkness is not dark to you;
the night is bright as the day,
for darkness is as light with you. (Psalm 139: 7-12)

































 The conclusion of Allistaire’s biopsy is well, sort of inconclusive. What we can say definitively after a week of numerous tests on the sample from her lungs is that it is not leukemia, not fungus and not bacteria. Obviously this is all good news, actually fantastic news! However, there is something going on in there. We seem to be down to two remaining possibilities not previously considered. Either the spots are evidence of a recovering infection or are evidence of Cryptogenic Organizing Pneumonia (COP). The cells are described as hemosiderin laden macrophages. Actually, the description of the tissue is far more detailed than that – I will include it below just so you can be in awe of both our amazing bodies and of the task of the pathologist. In a way it would be surprising if the spots are evidence of a recovering infection given that they were not present on the previous CT, nor has she had any symptoms. On the other hand, the sort of COP that Allistaire could have is actually a complication of a bone marrow transplant typically seen in adults and is a process of GVHD (Graft Versus Host Disease). Allistaire did have COP in the spring of 2014 and was successfully treated with steroids. Again, Allistaire has absolutely no symptoms of anything happening in her lungs, just this sole indication derived from the CT.
The conclusion of Allistaire’s biopsy is well, sort of inconclusive. What we can say definitively after a week of numerous tests on the sample from her lungs is that it is not leukemia, not fungus and not bacteria. Obviously this is all good news, actually fantastic news! However, there is something going on in there. We seem to be down to two remaining possibilities not previously considered. Either the spots are evidence of a recovering infection or are evidence of Cryptogenic Organizing Pneumonia (COP). The cells are described as hemosiderin laden macrophages. Actually, the description of the tissue is far more detailed than that – I will include it below just so you can be in awe of both our amazing bodies and of the task of the pathologist. In a way it would be surprising if the spots are evidence of a recovering infection given that they were not present on the previous CT, nor has she had any symptoms. On the other hand, the sort of COP that Allistaire could have is actually a complication of a bone marrow transplant typically seen in adults and is a process of GVHD (Graft Versus Host Disease). Allistaire did have COP in the spring of 2014 and was successfully treated with steroids. Again, Allistaire has absolutely no symptoms of anything happening in her lungs, just this sole indication derived from the CT.

























































































































































{kind=link}