









 You look out upon a field studded with rocks, rocks small that huddle together in the hand like eggs in a nest, fist-sized rocks, rocks you think if you gave them all your strength you could heave up out of that earth, hold to your chest, hugging them round with your arms. And here and there, a few scattered boulders. Boulders, monoliths, enormities that stand silhouetted against the sky.
You look out upon a field studded with rocks, rocks small that huddle together in the hand like eggs in a nest, fist-sized rocks, rocks you think if you gave them all your strength you could heave up out of that earth, hold to your chest, hugging them round with your arms. And here and there, a few scattered boulders. Boulders, monoliths, enormities that stand silhouetted against the sky.
How can I ever gather them all? The task overwhelms. Scattered all about they don’t look like much. Yet to convey the enormity of the day, one massive boulder would never suffice. No, all those rocks would be necessary. And not just a great pile, no, no, an intricately designed wall. Or better yet, something yet more complex: a dome formed with each rock set carefully in place. Rock against rock. Force pressing up against force. Rocks tucked tight so that the tension could somehow hold up the curvature.
To come to this day, this day seemingly like hundreds of others, has required a hundred thousand minute steps. How many times has a nurse “entered” her line? Fifteen seconds of scrub time. Fifteen seconds of dry time. How many sets of vitals? How many CBCs (Complete Blood Count)? How many echos and bone marrow biopsies? How many times have her cells gone hurtling past a laser, striking that electron off to release a burst of energy at a precise wavelength to reveal its identity? How many transfusions of red blood and platelets? How many emails flying back and forth between doctors, careful to consider all facets of her case, what will be best? What meds? What protocols? How many great hurdles overcome? How many slim possibilities made real?
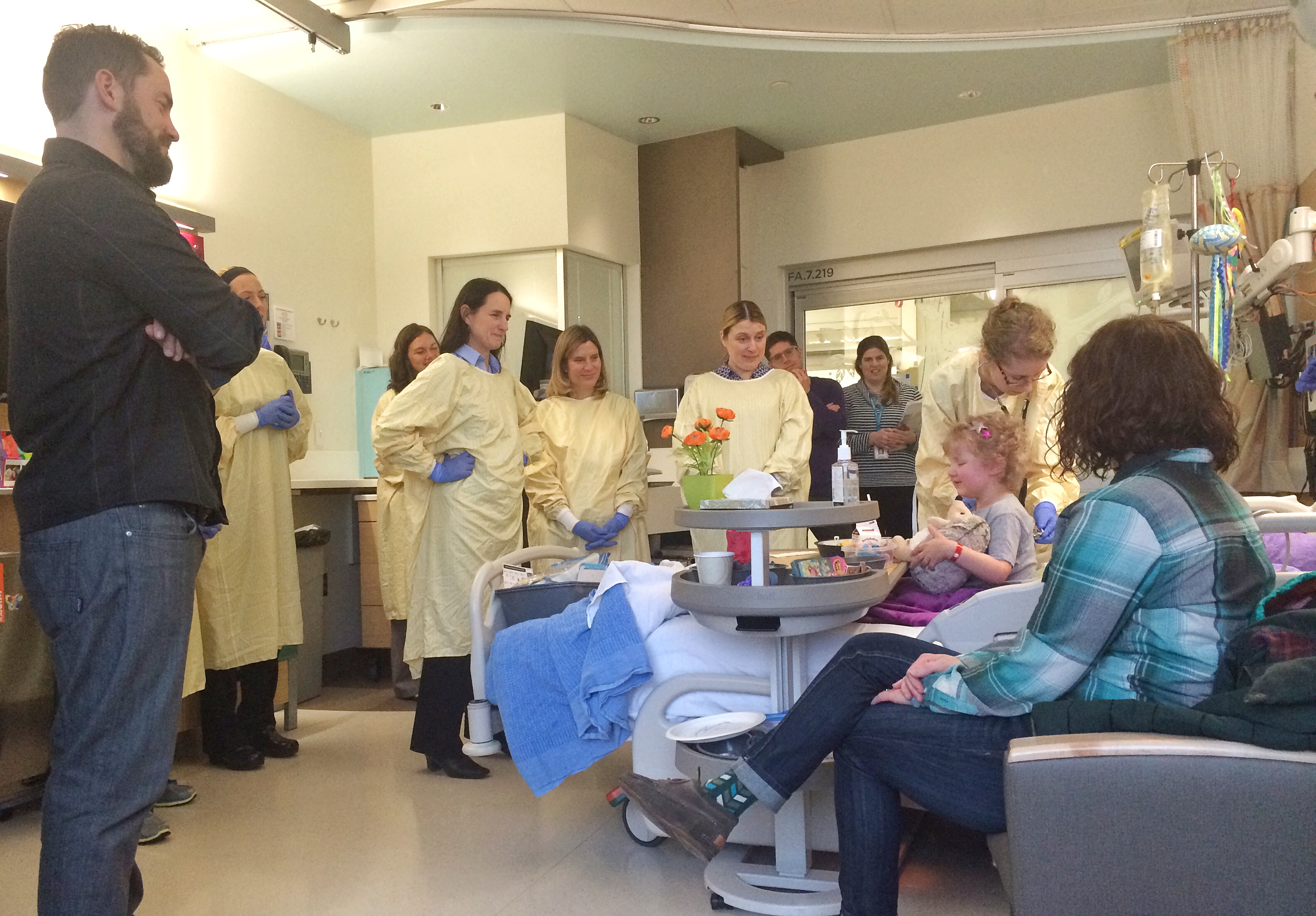
When at last the time came, when at last word came that, “the cells are here,” and the room began to flood with folk, tears came quick. Tears of being just plain overwhelmedly grateful. The weight of the bounty, the absolute wonder of all that has taken place to bring us to this day. This day. This day of transplant. This day of hope, of an open door, of another gift, another opportunity to pull a weapon from the scabbard and thrust it into the heart of those cancer cells. And the faces…faces dear to us, faces with whom the most difficult possible conversations have taken place. Faces beaming with joy for having walked long segments of this road with us. And though the faces of many were not present, I saw them still. In my mind there I saw Dr. Pollard, Dr. Gardner, Dr. Tarlock, Dr. Cooper, Dr. Berstein, Dr. Law, Dr. Kemna, Dr. Hong, Dr. Albers, the faces of countless nurses, of pathologists, and lab techs, Mohammed and Bonnie. The list could go on and on. If this was a Golden Globe I’d be kicked off the stage.
And there was something so poignant about the setting. The plan had been all along to put Allistaire in the ICU for the most crucial, dangerous portions of transplant. The ICU has many more means of monitoring her heart and an array of cardiac meds that cannot be given on the Cancer Unit. Allistaire cannot be handled by standard protocols alone. Everything that happens with intense immune responses result in the potential for great fluid shifts which in turn can radically impact the heart. The first event of concern was simply receiving her cells. As with all blood products, there is always the risk of an allergic type reaction, but even more significant is the possibility of a “cytokine storm,” due to the large mis-match between Sten’s stem cells and her own body. It is like two great waves crashing into one another. This clash of contrasts can result in a cascade of immune system signally and response that can be severe enough to be fatal.
When I asked the nurse what room we would be in the ICU, my mouth dropped at her response. Forest PICU 6 room 321. The very room we spent 70 of the 80 days Allistaire was in the PICU last January through April. So as the morning turned to afternoon and the cells finally began to flow into her line, and the “Happy Transplant Day,” song was ended, and someone yelled, “Speech!” – I simply could not resist. I could not resist proclaiming the wonder that we had come full circle, that in the span of one entire year, we had returned to this very room to at long last enter this gauntlet of transplant. As I stood there before that little throng of medical staff and family, the bare white unadorned walls of this agonizingly familiar ICU room constraining, my heart was bursting, my few words fumbling to offer up a naming of gift and thanks. Thanks for each person present and not present who has so faithfully, and graciously and compassionately done their part. We have each put our head into the wind and pressed forward though relentlessly buffeted, somehow forward motion has been attained and as we look back, wow, wow, who can believe we have covered such a great distance?!
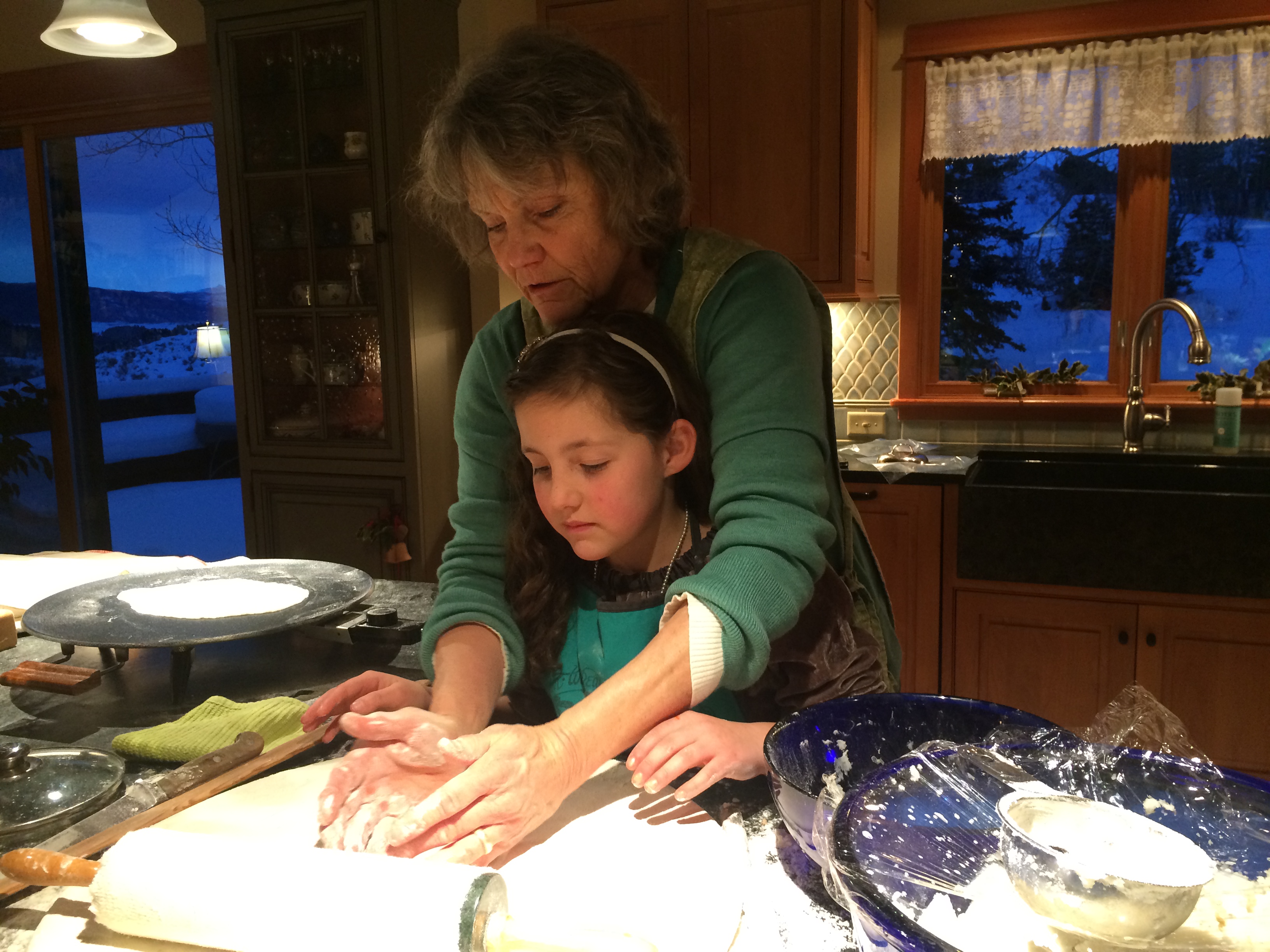
In the center of the room, a bright flash of spirit. Allistaire Kieron Anderson, a spirit whose light is like sparkling pink lemonade, giddy, curls upon curls, curls of blonde hair tinged in pink and curves of cheek and chin with light glinting out of her blue eyes. Lord, you make a crazy claim, one hard to fathom, sometimes hard to swallow, yet simultaneously gorgeous and wondrous: You know all of our days before one of them comes to be (Psalm 139:16). I have sought your face, I have yearned to walk this life held in You and one year ago, you said, “Come, follow Me, take my hand and let us walk this way, down this road leading into darkness,” as alarms blared on pumps and CT scans and echocardiograms declared disaster. I don’t know the road ahead, but as I turn, craning my neck back to look down that dark road behind me, hand gripped in Yours, I am simply in awe, in awe of the dangers and sorrows, of tears that threatened to drown and always Your hand, never letting go, and always Your Word, Your quiet voice entreating me to fix my eyes on You, on You and rest child, rest, rest in Me though all around you, you feel the ground giving way and the night presses in thick and you can’t seem to catch your breath, and the teeth flash and your whole being groans.
And startlingly, here we are, we have circled back around. The obvious question is, “Why? Why Lord? What was the point of all that? I mean really, really, did we really have to take what feels like a year-long detour through treacherous territory only to come back to where we started yet more bloodied and bruised, wounds deep?” So much lost. So much time. So much separation. So much damage. So very many tears. The lacerations and scars are easy to see yet don’t begin to reveal the depth of ravaging. What is harder still to see is the other-worldly beauty, the treasure often imperceptible. Seeds in dirt don’t look like much. Seeds sailing on winds…The Lord’s aim has never been transplant. He aims for my heart, for all hearts and sometimes in great peril and pressing darkness we are more able to see aright, to incline our ear to His voice, to have His Word made full and pulsing with life, our stiff necks bend low and we come to worship the God of creation as never before. Getting to transplant has never been hard for the Lord. To say that it has been trivial in His sight sounds callous only when I fail to set it against the enormity of His heart for me, for me a child of Adam, a child of God. But I have no doubt God smiled broad and His face beamed as we gathered in that small room and were witness to the marvel of the human body, to the tenacious brokenness of creation, to the wonders of medicine and human endeavor, and to hope, hope for a way through.
I don’t know the road ahead and there is the quiver of trepidation, knowing there are still many dangers. But on this gray January day with rain intent on saturating, my heart feels heavy and full, full with the satiation of joy and full of yearning to keep leaning in, inclining my face to the face of my God. I look at this little girl and marvel that I should be so blessed to call her daughter and to walk this road with her, to hold her sweet little hand along the way, and to incline my ear to the pleasure of her small sweet voice, a voice proclaiming dreams of a future and joy for the present, delight in simply putting color down on paper, color alongside color alongside color.
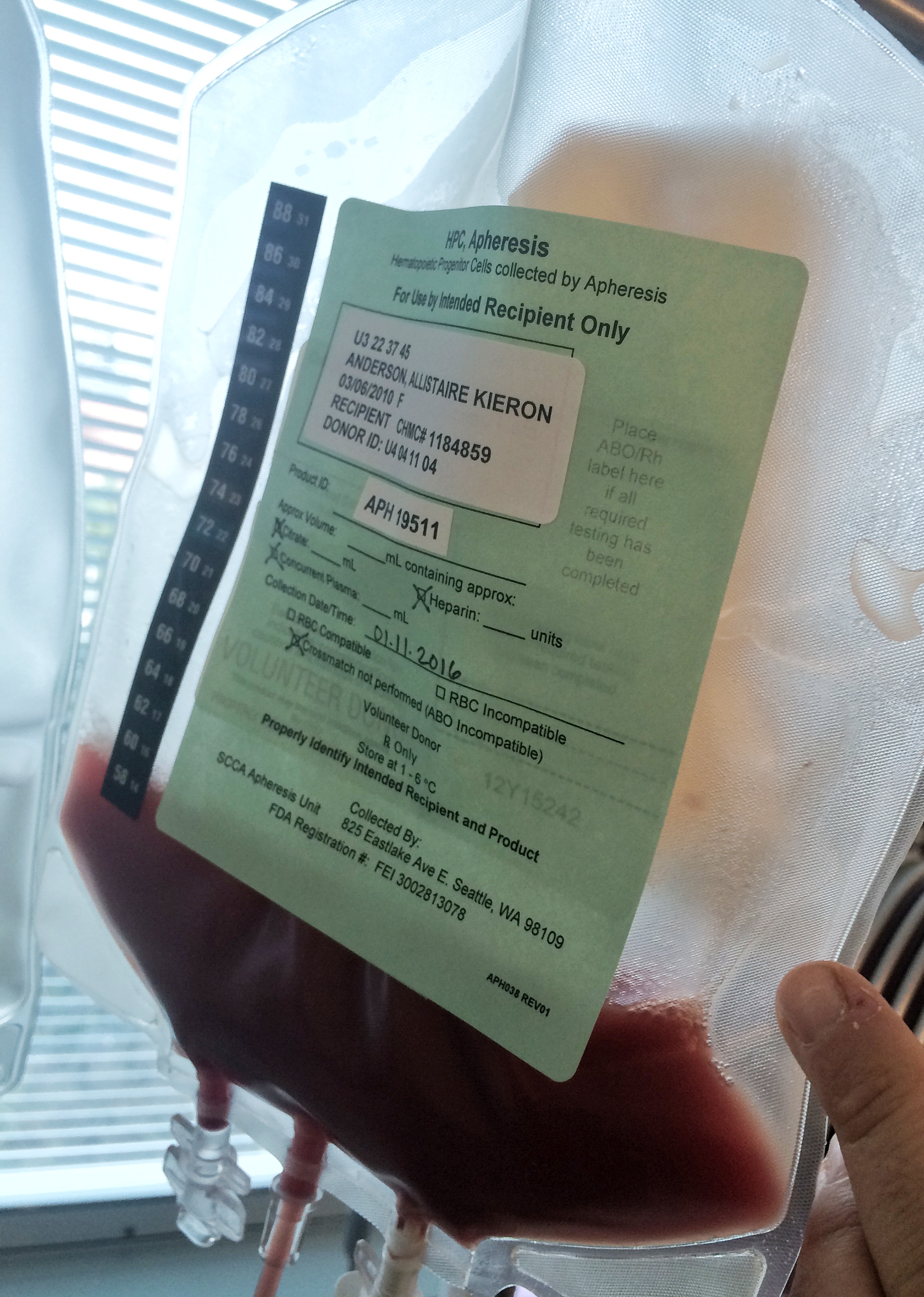
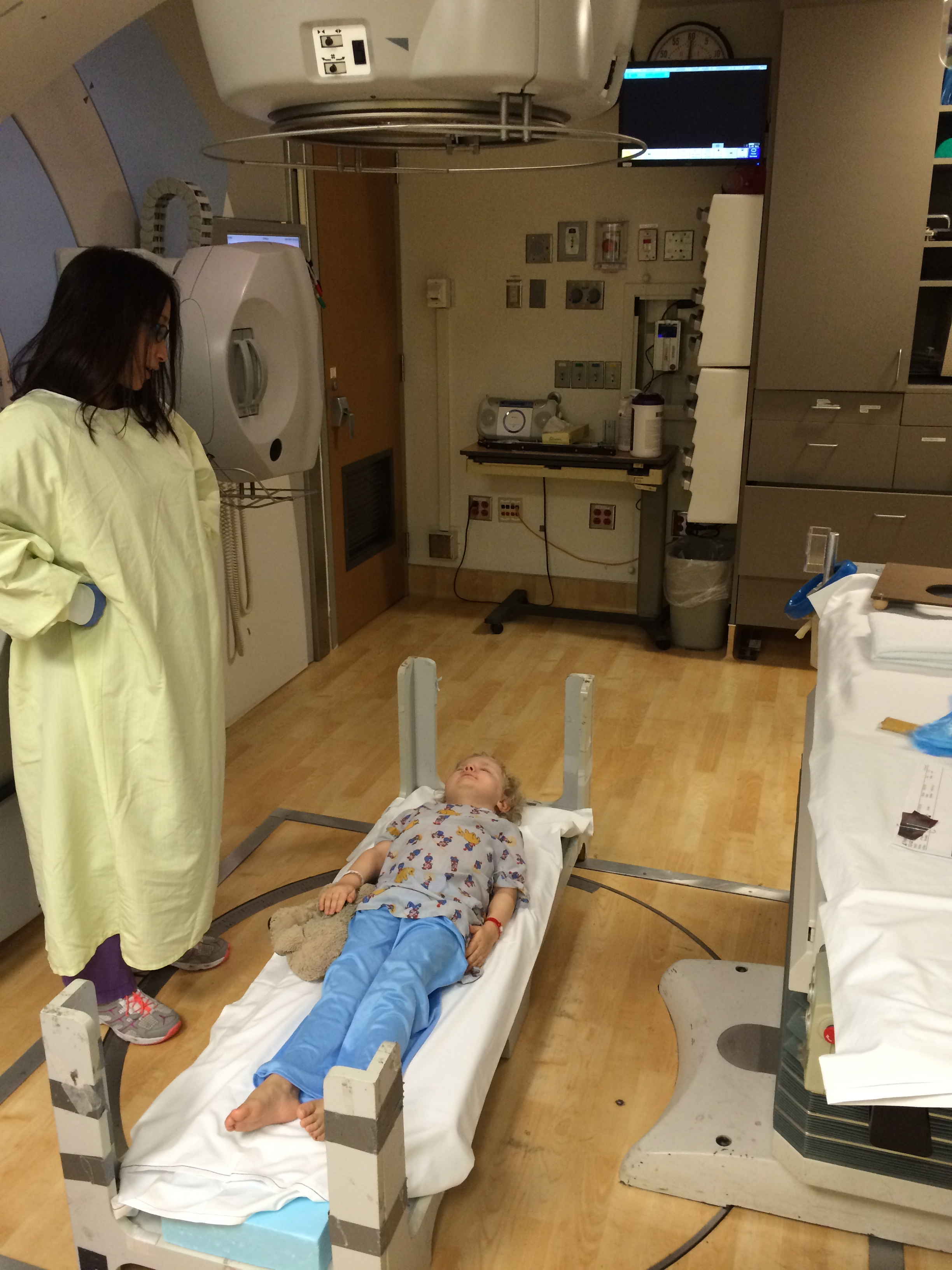
Allistaire has made it through five fractions of focal radiation to the chloromas in her sinuses, eight fractions of TBI (Total Body Irradiation), three doses of the chemotherapy Fludarabine, all in preparation, a “conditioning,” for transplant. The only direct immediate result has been fatigue and a C-Diff (Clostridium Difficule) infection due to the effects of radiation on her gut for which she is now on Flagel. On Monday, on her day of rest, Sten’s birthday, Sten received his fifth and final shot of GCSF (Granulocyte Colony Stimulating Factor). Then, in the early afternoon over the course of several hours, his blood was pulled out, and through the action of centrifugal force, the lighter weight white blood cells including CD34 stem cells, were separated out and the remaining blood returned, a process known as apherisis. In total, the goal of 5-6 million CD34 cells/kg was achieved in a mere 187ml of Sten’s blood. Sten’s blood was then processed, having both the red blood cells and platelets removed because of the antibodies Allistaire has formed against them. When that bag of orangish red blood arrived in Allistaire’s room on Transplant Day, it contained nearly 120 million CD34 stem cells within 148 ml.
Due to extreme weariness at countless plans dashed, I felt no need to explain this transplant of Allistaire’s until it actually came to fruition. So at last it is clearly time to explain what we’re doing here because truly there are so many different types of bone marrow transplants, each specially designed and chosen to fit with the uniqueness of the patient and their disease. In order to make any sense of what is happening in Allistaire’s transplant, a brief overview of bone marrow transplants seems necessary. When transplants were first developed by Dr. Donnall Thomas of Fred Hutchinson Cancer Research Center in the 1960’s and 70’s, the goal was to have the ability to use extreme doses of chemotherapy and radiation to destroy a leukemia patient’s bone marrow, the source of their cancer, and then “rescue” them by giving an infusion of another person’s bone marrow. Without this “rescue,” the obliterated marrow could never recover and the patient would die. Only later was it discovered that a key component of a bone marrow transplant’s potential to cure comes from the immunotherapy effect of Graft Versus Leukemia (GVL). More about that in a bit.
All bone marrow transplants begin with “conditioning,” which primarily attempts to eradicate any remaining cancer cells and to make way for the incoming stem cells. Patients have the highest chance of a “successful” transplant when they go into transplant in remission which is generally defined as little to no detectable disease. In Leukemia this means 5% or less disease in the marrow and ideally no extramedullary disease (cancer cells which form tumors outside of the marrow). Each transplant protocol has specific requirements regarding disease status which determines whether or not a patient will be approved to move forward with a transplant. Additionally, there are numerous conditions of health, especially regarding the major organs (heart, liver, kidneys, etc). Determining which specific transplant regimen is best for the patient requires a great deal of data gathering and consideration. All have variable elements of benefit and risk.
The two key defining components of a bone marrow transplant are the type of conditioning and the stem cell source. There are a number of different types and doses of chemotherapy which may be used in conditioning. Additionally, a patient may or may not also receive radiation as part of conditioning. Sometimes the radiation is focused only on certain areas of the body where there have been or are tumors, or only the lymph nodes may be targeted. In Allistaire’s case, she had both focal radiation and TBI (Total Body Irradiation) which sends radiation throughout the entire body. Depending on the patient’s health, they may or may not be able to endure full intensity conditioning. For older transplant patients who may not be in optimal health, “mini transplants,” were developed by Dr. Rainer Storb, also of Fred Hutch Cancer Research. In patients like Allistaire who have one or more major organ systems that have been compromised, intensity of conditioning is an enormous consideration. While Dr. Bleakley was very hesitant to give Allistaire a full-intensity conditioning transplant given the status of her heart, the extreme aggressiveness of her disease necessitated this in order to give her any chance of a cure.
The second component that distinguishes a transplant, is the stem cell source used for “rescue” after the marrow has been decimated. This might be may very favorite part of transplant. Rescue. A word conjuring up vivid, dramatic images, harrowing situations, bravery, sacrifice, love. To read specifically about about the beauty of “rescue,” as I wrote about in Allistaire’s first transplant click HERE. Originally, all transplants used whole marrow as the stem cell source which meant all donors had bone marrow removed directly from their bones. In time, a method was developed for harvesting stem cells from the peripheral blood with the aid of GCSF (Granulocyte Colony Stimulating Factor). GCSF promotes the production of stem cells in the marrow and their mobilization into the peripheral blood where they are collected by apherisis. This is the means by which Sten donated his stem cells. Lastly, the most recently developed stem cell source is that of cord blood. Cord blood is blood that is extracted from the umbilical cord of a newborn baby. Mothers can opt to donate their child’s cord blood which is then registered with the National Marrow Registry and banked, awaiting a person in need of a transplant. It should be noted that some cancer patients have their own stem cells harvested and then reinfused after conditioning. This type of transplant is known as an Autologous transplant. However, whenever a particular blood cell line itself is the source of a patient’s cancer, as in the case of leukemia, they cannot be “rescued,” with their own stem cells as these are the source of their cancer. In an Allogeneic transplant, the patient receives another person’s stem cells.
Many clinical trials have been conducted exploring the risks and benefits of diverse combinations of conditioning regimens and stem cell sources. However, a major consideration in determining what type of stem cell source to use in a patient’s transplant is simply availability. To receive someone else’s bone marrow fundamentally means you are receiving another person’s immune system. Our immune system is able to accomplish the extraordinary defense of our bodies in large part because of its ability to identify “self” and “other.” This is actually why cancer is so hard to eradicate. In essence, the immune system of a person with cancer has failed to identify their cancer cells as “other.” This is because cancer cells develop from normal healthy cells. The goal of virtually all cancer treatment is to discern and target the subtle differences between healthy cells and cancer cells. Typically a prospective transplant patient is “matched” to the greatest degree possible with the incoming stem cells so that the incoming cells look as close to “self” as possible. This is done through HLA typing. On human’s chromosome 6, there is a grouping of genes that encode for Human Leukocyte Antigens (HLA) which are then presented on the cell surface of all cells in a person’s body. It is like a bar code (in the form of cell surface proteins) used as a unique identifier for that person. These HLA proteins are what distinguish one individual person from another and are what allow a person’s immune system to identify “self” from “other.” The immune system aims to identify and destroy anything “other.” For this reason, it is essential that there be a significant degree of HLA matching between the patient and the incoming stem cells. Otherwise, the patient’s own immune system would heartily attack and destroy the incoming stem cells. When this happens it is known as “graft failure.”
Another potentially severe complication of a HLA mismatch between patient and donor is known as GVHD (Graft Versus Host Disease). In this situation, the incoming donor cells may identify the patient’s body as “other” and set about attacking the patient’s tissues, most commonly the skin, gut and liver. GVHD can even be fatal. The ways to prevent or reduce GVHD have typically been to select the highest degree of HLA matching and/or give the patient immune suppressants which suppress the immune fighting T-cells within the graft/donor cells. A major down side of immune suppressants is that they also suppress the incoming immune system’s ability to fight infection which can often lead to life-threatening infections. As research into GVHD progresses, scientists are learning more about what subsets of T-cells are responsible for the majority of GVHD. Dr. Bleakley has been conducting a clinical trial in which the “naive T-cells” are depleted or removed from the donor cells prior to infusion into the transplant patient. This has succeeded in substantially reducing the incidence of chronic GVHD. Click HERE to read more about this fascinating research yielding substantially better results.
The highest degree of HLA matching is a 10 out of 10 match, which means the patient’s cells share the same genetic code as the donor cells at the ten major points on Chromosome 6. In order to accomplish this matching, patient and donor most often share very similar ethnicity. It is more difficult to find a good match for those patients who are ethnically diverse, whose ethnicity is rarer or derives from parts of the world in which there is very low Bone Marrow Registry participation. For example, one of our friend’s was from the indigenous tribes of Guatemala. Her specific ethnicity is simply rare in the world. Another friend with sickle-cell was Ugandan, a part of the world with very little registry participation. Almost amusingly, in Allistaire’s case she may be “too white,” in that she has never had a single match within the United States. Her matched donors have always been found through the German registry. She was unable to participate in Dr. Bleakley’s naive t-cell depleted protocol because it requires a U.S. donor. For this reason, patients will have better transplant options when more people join the Bone Marrow Registry, thus increasing the likelihood that the patient can find a match. For patients who have no sufficient bone marrow matches, cord blood can be a good option because it must be matched at fewer points (max of 6 out of 6). Again, this is why donating your newborn’s cord can literally save a life!
As noted, the two major distinguishing components of a stem cell transplant are the type of conditioning and the type of stem cell source. There is no one right transplant as each patient comes into needing transplant in varying degrees of health, disease status and access to stem cell source. Allistaire went into her first stem cell transplant in June 2013 with nearly 70% disease in her marrow and 9 chloromas/tumors. Otherwise her body was “healthy.” Nevertheless, because of the enormity of her disease, she was only able to receive a transplant because of a specific transplant clinical trial through Fred Hutch that did not require remission. She would have been dead long ago had it not been for that clinical trial. When Allistaire relapsed again in October 2014 and needed a second transplant, we were aiming to use the “naive T-cell depleted transplant,” which did require remission. Fortunately remission was attained but Allistaire had no U.S. matches and Dr. Bleakley set about trying to gain permission from the FDA and the German registry to allow Allistaire to use the available matched German donor from outside the U.S.
However, last January the cumulative effect of her years of chemotherapy and the severe typhlitus infection put her into heart failure. She no longer qualified for transplant because of the extremely poor function of her heart which nearly resulted in her death. Even once she regained some function, for a very long time she would have only qualified for low-conditioning transplants. However, no low-conditioning transplant could sufficiently wipe out her extremely aggressive disease. So for the past 10-11 months the goal has been to keep her cancer under control while giving her heart the time to possibly regain enough strength to qualify for a full-intensity conditioning transplant. This has been extremely difficult as the oncologists have had limited treatment options. Many types of chemotherapy themselves can be hard on the heart and/or greatly assault the marrow, effectively suppressing the immune system which then allows for the possibility of life-threatening infections. Not only can the infection itself kill you, but the body’s attempt to fight the infection often causes major fluid shifts, changes in heart rates and blood pressures, all of which can put major strain on the heart. Even seemingly minor situations like the two instances of an ileus resulted in all her medications, fluids and sustenance being given IV which puts a great burden on the heart. It is a tough situation all around. This was the reason for trying the WT1 modified T-cells and the decision to try Mylotarg (available only on a compassionate-use basis through Fred Hutch). And while the Mylotarg was impressively effective against Allistaire’s cancer, one problem has been the incidence of cancer cells mutating in resistance to it and the risk of causing SOS (severe liver complication) in the context of transplant (which is why it was pulled by the FDA in 2010).
Once Allistaire’s heart began gaining strength as evidenced by ejection fractions (as determined by echocardiogram) in the high 30s and low 40s, the discussion began in earnest as to whether or not it might finally be time to give one more great thrust toward transplant. Countless conversations between the Oncology, Bone Marrow Transplant and Cardiology doctors debated risks and benefits which were strongly tied to both keeping her disease under control long enough to get to transplant and what transplant regimen could give Allistaire the best chance at a cure and not kill her in the process. When Dr. Bleakley first suggested the real possibility of a Haplo transplant, my gut response was to spit that idea right back out. A Haplo-identical transplant is one in which the patient is half matched (5 out of 10) with a parent or sibling.
Because of this extreme mismatch, Haplo transplants have historically been associated with many poor outcomes including graft failure, high incidence of severe GVHD, high rates of infection and relapse. Each awful complication results from attempts to respond and mitigate one of these other complications. For example, because the HLA is only half matched between patient and donor, the patient’s immune system can attack and wipe out the graft/donor immune system. Graft failure can be mitigated by increasing the intensity of conditioning to suppress the patient’s own immune system. However, there is still the likelihood of severe and/or chronic GVHD where the donor immune system attacks the patient. In order to combat this, the patient is given immune suppressants to tamp down the immune response in the donor cells. This in turn results in severely lessened ability to fight infection and may reduce the Graft Versus Leukemia effect which is the advantageous and desirable element of the mismatch between “self” and “other.” Remember that because cancer cells derive from healthy cells, they carry the HLA typing of the patient so when donor cells come into the patient’s body, they are more able to recognize the cancer cells as “other” and destroy them. Dr. Bleakley provided me with this paper, (Modern Approaches to HLA-haploidentical blood or marrow transplantation), which gives a historical overview of Haplo transplants.
Dr. Bleakley went on to describe a more recent approach to Haplo transplants which has yielded results on par with that of standard unrelated-matched donor transplants. The most unique aspect of this transplant is that the extreme mismatch between patient and donor (half-matched parent or sibling) which would naturally produce immense GVHD, is greatly mitigated by giving a strong dose of the chemotherapy, cyclophosphamide (also known as Cytoxan), on days 3 and 4 after the infusion of the donor cells (the actual day of transplant). This also occurs in the absence of any immune suppressants which are traditionally started at Day-1 (the day before transplant which is known as Day 0). What this means is that when the donor cells go into the patient’s body, there is an uproar of immune systems in which the donor immune system begins to respond to the presence of “other” by rapidly dividing its Tcells and beginning the process of fight or GVHD. There is nothing to lessen this response of the incoming donor cells because there are no immune suppressants present. This is where the possibility of a cytokine storm comes in and where severe GVHD could take off if there was no intervening. The possible cytokine storm must simply be managed as best as possible but the revving up of the donor Tcells is stopped in its tracks by these two large doses of cyclophosphamide on Day+3 and +4. The cyclophosphamide targets rapidly dividing cells including the Tcells, which left unchecked, would produce immense GVHD. The way that the whole graft/donor cells are not altogether wiped out by this chemo is that, according to a recent discovery, stem cells have proteins on their cell surfaces which make them immune to this particular chemo. Also left, are a subset of Tcells which were not highly activated and can still go on to fight infection and provide GVL (Graft Versus Leukemia). There are various versions of this “post-transplant Cy.” Allistaire’s includes TBI (Total Body Irradiation) in the conditioning portion of the transplant which is essential given the aggressiveness of her AML and the ongoing presence of extramedullary disease. Other “post-transplant Cy,” transplants may have reduced intensity conditioning. Dr. Bleakley followed a transplant regimen based on the research described in this article (Total Body Irradiation-Based Myeloblative Haploidentical Stem Cell Transplantation in Patients Without Matched Sibling Donors), published in July 2015.
So at long last we come to this week of transplant. And for those of you with eyes glazed over or simply head asleep on the keyboard, part of my motivation in going to such lengths to explain this transplant is not only for my own documentation, but also for folks out there in situations like ours who may need detailed information. Given the condition of Allistaire’s heart and the aggressiveness of her disease, we therefore, chose a transplant with full-intensity conditioning and most importantly, full dose TBI which you can only have once in a lifetime. The reason for choosing Sten as Allistaire’s donor is for three main reasons. First off, Allistaire’s chance of both surviving transplant and having it actually cure her is extremely low and so ethically, the doctors do not feel right about asking an unrelated donor to undergo risk and burden to be her donor. Secondly, given the highly fluctuating nature of Allistaire’s health and disease, the projected date of transplant could easily change which might mean we lose our donor who has constrained availability and requires more pre-planning because they would be donating on the other side of the earth (remember no U.S. donor matches). Sten, as Allistaire’s father, is more than willing to take on risk and burden and is a highly committed and extremely flexible donor. By the way, both he and I were options but it was concluded he was the better choice. Lastly, the statistics for acute and chronic GVHD, NRM (non-relapse mortality), relapse, DFS (2 year Disease Free Survival) and OS (2 year Overall Survival), were on parr with the statistics for standard unrelated-matched donor transplants. This means that we have the opportunity to give Allistaire as good of a chance at survival and a cure with her dad as a half HLA matched (haplo) donor as she would with a fully matched 10 out of 10 HLA matched unrelated donor with the added benefit that comes with having your awesome dad who is willing to literally lay down his life for you.
Thus far, Allistaire has received her infusion of Sten’s stem cells, essentially getting her transplant on Tuesday, January 12th. She had no allergic reaction to the cells. However, later in the evening she had a fever with higher heart rates. Whenever an immune suppressed patient (in her case because of conditioning, not immune suppressing medications), gets a fever, blood cultures are drawn and antibiotics are started in case the fever is evidence of an infection. Thankfully, Allistaire’s fever seems only related to her response to the mismatch of the incoming donor cells. Dr. Bleakley was quite pleased as the fever was evidence of an immune response without the danger of a full on cytokine storm.
In the last few days, Allistaire has started to get some mouth sores, an expected result of conditioning which especially impacts rapidly dividing cells. This means all the cells lining the digestive tract from the mouth all the way out the other side are hit hard. This can result in mucoscitis. She is more gaggy and nauseous, has thrown up a few time and has begun to eat far less. At this point we are prioritizing her drinking the necessary fluids and continuing to take her oral meds, (rather than giving her IV fluids and IV meds which would be harder on her heart). We are attempting to have her drink a pint of milk at each meal time to provide some calories in the form of protein and fat. She may soon require her nutrition to be converted to TPN and lipids which are essentially IV forms of sustenance.
The next storm on the horizon begins tomorrow with the two days worth of cyclophosphamide infusions. A side effect of cyclophosphamide can be bladder bleeding which they try to counteract with hyper-hydrating and a medication called Mesna. Because of Allistaire’s weaker heart, they are reducing the hydration from the standard 1.5 times maintenance to 1.25 and are hopeful that this will both be enough to prevent the bladder bleeding and not overwhelm her heart. Another serious and potentially fatal, but rare, possible side effect of cyclophosphamide is acute cardiomyopathy due to hemorrhagic myocarditis. Depending on how things go, Allistiare could be transferred from the ICU back to the Cancer Unit early next week.
Honestly, it is an absolute wonder that she ever made it to this transplant. Whether or not she will survive the transplant or it will be successful at curing her of her cancer are totally separate questions. I am just simply in awe that we are here. The Lord will continue to be faithful, morning by morning, come what may.
To join the Bone Marrow Registry, go to Be The Match
Learn about how to donate your baby’s cord blood


































 Cacophony
Cacophony






































































































































































































{kind=link}
{kind=link}
{kind=link}
{kind=link}