 I used to think I was safe, that wild animals, the beasts, the possibility of having my flesh torn off of bones, lay up there, out there, far off in dark mountainous woods. I thought it would be easy to simply steer clear of such terrors. As though somehow my own willing of my footsteps could keep me from entering their realm, that by hope, optimism, some silly assumption of impenetrability, it would not be so hard to keep those ravages at bay. I walked in a sunlit land, blithely believing, perhaps not even believing but never even thinking that they might tear down the hillside at terrifying speeds, absolutely bent on destruction. They do not see a heart full of hopes, of dreams, of ideas, of lists of yearnings, eyes bright. Their horrible feet carry them, saliva flinging back behind as their daggers flash, crazed eyes.
I used to think I was safe, that wild animals, the beasts, the possibility of having my flesh torn off of bones, lay up there, out there, far off in dark mountainous woods. I thought it would be easy to simply steer clear of such terrors. As though somehow my own willing of my footsteps could keep me from entering their realm, that by hope, optimism, some silly assumption of impenetrability, it would not be so hard to keep those ravages at bay. I walked in a sunlit land, blithely believing, perhaps not even believing but never even thinking that they might tear down the hillside at terrifying speeds, absolutely bent on destruction. They do not see a heart full of hopes, of dreams, of ideas, of lists of yearnings, eyes bright. Their horrible feet carry them, saliva flinging back behind as their daggers flash, crazed eyes.
Flood waters tearing homes in half, separating husband and wife with children. Father of Solveig’s classmate, life cut short from heart attack. Jens on a mountainside. Nine year old girls sold into slavery by Isis. Kassidae home from yet another T-cell trial that utterly failed to stop her cancer.
What is it like to have no more options? How can I fathom a journey where suddenly the road simply ends. No destination reached, just a faint trail blending into nothing, melding into the landscape. And then what? And then what? Where does one go from there?
I see a small child standing alone in an open space. Nothing in their hands. No clothes. No defense. Utterly vulnerable. I stand and watch, unable to move, unable to raise my hand to stop what I know will come, what is coming.
The child shivers, confusion in their eyes. And then you sense it, before even sound reaches your ears. Some sort of terrible rushing, some silent invisible foe rushing through the forest. At last it breaks through the trees, snarling, feet hardly touching the ground as it bolts for your child, savage mouth wide. And do you turn away? Can you stand to watch the beast tear into your child’s flesh? Dare you know the moment their life is extinguished? How much will be ripped and torn before their eyes go limp and lifeless?
I heard these words in a beautiful song, a song meant to comfort, a lullaby.
“Quiet your heart
It’s just a dream
Go back to sleep
I’ll be right here
I’ll stay awake as long as you need me
To slay all the dragons
And keep out the monsters
I’m watching over you
My love is a light
Driving away all of your fear
So don’t be afraid
Remember I made a promise to keep you safe
You’ll have your own battles to fight
When you are older
You’ll find yourself frozen inside
But always remember
If you feel alone
Facing the giants
And you don’t know
What to do
My love is a light
Driving away all of your fear
So don’t be afraid
Remember I made a promise to keep you safe”
My heart was breaking as I listened to these words. Hot silent tears slid down as I drove, facing forward, intent on the task of getting there. “You’ll have your own battles to fight when you’re older.” But no, no, Allistaire did not get to be older before she had her own battles to fight. She was just 21 months old when her battle against this ravaging beast first came, intent on taking her life.
“Mommy, I like that part, ‘you feel alone, facing the giants, and you don’t know what to do.” Her soft sweet voice came to me from the back seat. Of all the words in all the songs, these are the one’s she speaks out loud, repeats back to me, the words that most resonated with her little girl heart.
You think, unconsciously believe, that as a parent you can protect your child, that somehow, by force of will you can magically keep them from harm. Surely there is nothing more core to being a parent, to being a mother, than protecting the life of your child.
But my love, oh my love, so fierce, stuffed full with all my might and zeal, my hope…it is powerless to protect against some enemies. I never made that promise to keep her safe, I just assumed it would be true. Of course she will be safe. Of course I can wrap her up in a hug and overcome any giant.
No. There may come a time where there are no options left and I will hear the rushing of wind through branches as that beast comes tearing through the forest, breaks out into the opening and sinks its wretched brutal teeth into the one I love, this time sparing nothing. I may be left with my heart bleeding out in the open space, tattered, wounded, ravaged child in my lap, never again to see her bright eyes, never again to hear the most beloved sound on the whole earth, her laugh, her voice full of wonder.
But I know this. She will not stand alone. If such a time comes, I will stand with her, hand gripped in mine and I will face that beast with her. I will not turn away and I will not leave her, and that may be all that I can do. My eyes will weep until my own flesh is laid to rest.
To Shannon, to Kate, to Susan, to Becca, to Rachel, to Julie, to Beth, to Devon, to you many more mothers who have walked this road, who stood with your hand gripping your child’s as that beast came to devour, my heart weeps with yours and oh how I desperately long for a better day.
For those of you who know that Allistaire was discharged from the hospital almost two weeks ago, these words must come as a surprise. What you see on the surface is so far from the full story. People constantly comment, “She looks great!” They ask, “How is she doing?” How do I answer that question? On Monday at the playground, after having climbed up the slide twice in a row, Allistaire suddenly said she didn’t feel well, she was panicked and in pain but couldn’t explain what was really happening. There was terror in her eyes. I cradled her and hoped she would calm down. Maybe she just overexerted herself a little. She cried out in anguish, “Mommy,” over and over, yet I could not understand the source of her pain or her fear. I asked my five-year old daughter, “Do I need to take you to the hospital?” as though she could answer this question. Was she overreacting? What was she feeling? She threw up in the bathroom. Well, she was on day 6 of chemo and this was the first time she threw up, so really not concerning in itself. Of course nausea can be a sign of heart failure too. I scan through all I know in my head, assessing her energy, her sleep patterns, her appetite, food consumption. Could it be her heart? She continued to freak out after throwing up and we left the bathroom. “Mommy, can I feel the sand?” I took off her sandals and gently sat her feet down in the sand at Golden Gardens. Immediately she calmed. Immediately she was fine. What was real? What is true? How much of that was based on something of significance? How much is her just working herself up? I dreaded having to relay this incident to the cardiologists. It’s a lovely day at the park, but just below the surface are constant swirling realities that threaten to steal it all away.
In the first days of being out of the hospital, Allistaire and I gorged on our sudden freedom, on sunlight and bird song and starlight and bright moon, on playgrounds and sleeping without interruption, on hours of daytime without nurses and doctors and hospital food trays. Solveig and JoMarie arrived last Wednesday evening and my heart swelled with the joy of their laughter and heads clustered together in play. Everyday playgrounds, picnics and beaches, throwing rocks into water and sun glinting off lapping waves. Caterpillars on fingers and squealing. My faced beamed with delight, with wonder at simple ordinary life. How much more wondrous it is than people realize!
You think that leaving the hospital is some signal of victory, of progress, of normalcy. And so it may be, often is, though not always. We left on May 18th, not having accomplished what we came to do. In some ways the girl who left the hospital was worse off then the girl who came to Seattle back in October. The great victory was that she successfully weaned off Milrinone. A huge accomplishment which has made way for a few options, far more than none. But her heart is far too weak to endure a standard transplant for AML which includes TBI (Total Body Irradiation). So we left the confines of this hospital after 130 straight days, her only moments outside were the 30 seconds here and there strapped onto an ambulance stretcher as she was transported to and from The University of Washington for radiation. We went straight to the playground.
For 11 of the past 12 days since she was discharged, Allistaire has been to the hospital for a variety of appointments. On Tuesday the 19th she finished focal radiation to her left leg where one new chloroma (solid leukemia) showed up on her last PET/CT scan. On Wednesday she saw Dr. Todd Cooper, her new primary oncologist. Dr. Gardner is pregnant with twin girls and so we are making the transition to having Dr. Cooper, who is the newly hired head of the leukemia department and an AML expert. He is the doctor that Dr. Pollard had hoped would come to Seattle Children’s. He has been tasked with developing a High-Risk Leukemia program for Seattle Children’s. So when Dr. Gardner asked who I’d like to have as Allistaire’s new primary oncologist, it was a no-brainer to ask for Dr. Cooper, a kind man from Atlanta who is a super smarty pants AML doc. In our first outpatient visit with him, he relayed that Dr. Pollard had called him about Allistaire to make sure he was up to speed with all the details of her medical history. I cannot tell you how amazingly cared for I feel here at Seattle Children’s. We are blessed beyond words by the team that journey’s with us. After seeing Dr. Cooper, Allistaire began seven days of Azacitadine, the same chemo she got last time.
Prior to leaving the hospital, I met with Dr. Gardner and Dr. Marie Bleakley, the transplant doctor we’ve worked with at several significant points. It was really great to have them both present for the conversation. Dr. Gardner began with explaining her reasoning for waiting so long for Allistaire to begin chemo again. I had grown frightened with the incredible amount of time since her last round of chemo, knowing the immense need to keep her in remission and being aware that she was a month beyond the traditional time of starting a new round. Dr. Gardner stressed that because Allistaire’s marrow has been so incredibly slow to recover, her greatest immediate risk is that of an infection that one: she wouldn’t have the white blood cell defenses to fight and two: that could overwhelm her heart. So finally, nine weeks after the beginning of the previous round of Azacitidine, Allistaire would begin another round. She also stated again that given Allistaire’s heart, TBI, known to have long-term consequences to the heart, was not in her best interest at this time. Dr. Bleakley went on to describe a “midi-transplant” which has much lower levels of radiation (4 centigray as opposed to 12 in TBI) and heavy-duty myeloablative chemotherapy, and a “mini-transplant” with even lower levels of radiation (2 centigray) and non-myeloablative chemotherapy but high-dose steroids. I’ll forego going into the details of how each of these work and the pros and cons, but suffice it to say, the mini-transplant is not a good option as it is intended to extend life in the old who cannot endure hard-core conditioning. It is unlikely to provide a cure and has a lot of potential for GVHD (Graft Versus Host Disease). So while the “midi-transplant” is an option for Allistaire, with a gleam in her eye, Dr. Bleakley had a different proposal.
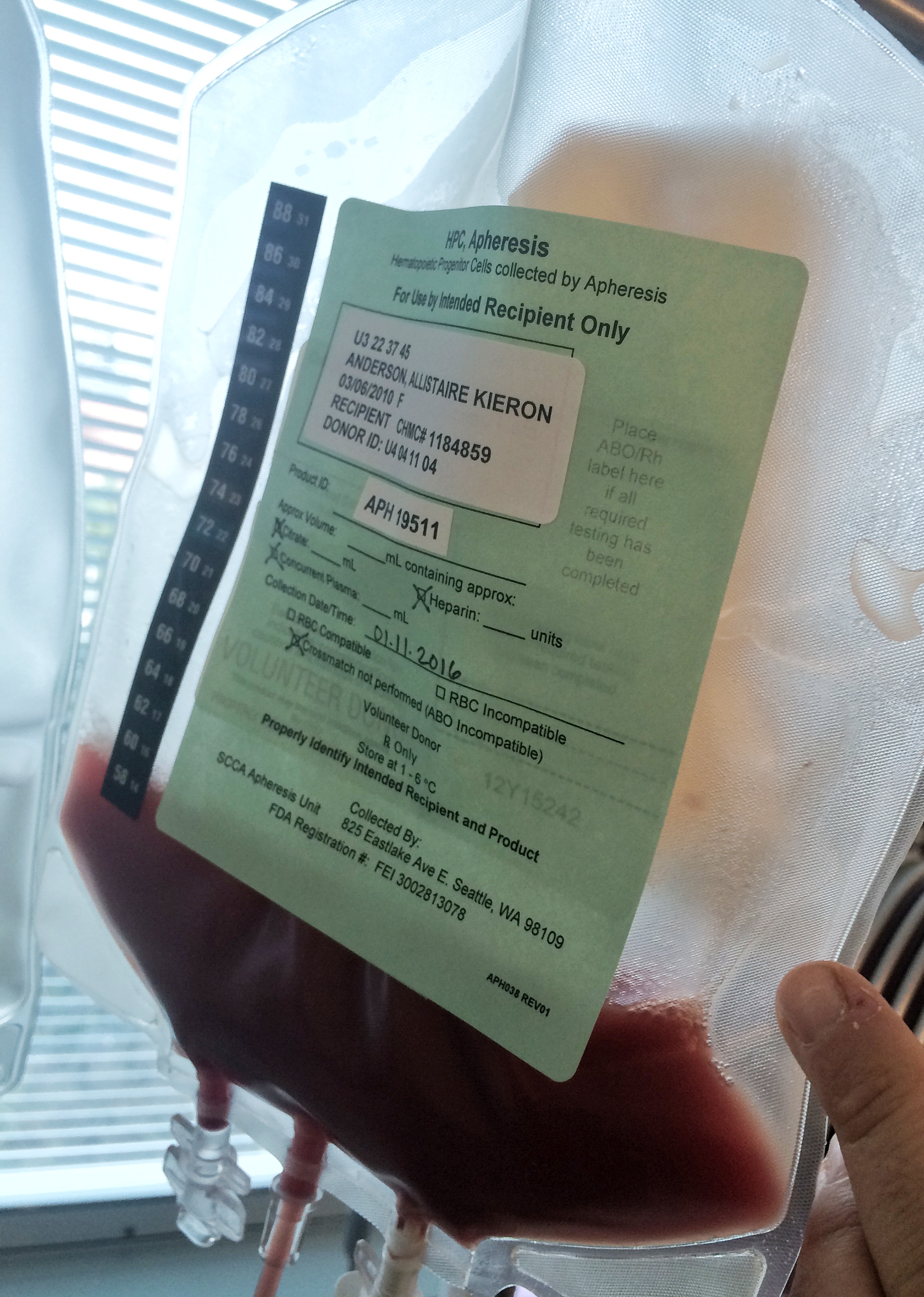
I left the room with hope. With fear yes, always there is fear, we walk ever into black, into unknown. But with hope, with a bit of upturned grin. Dr. Bleakley has proposed that Allistaire’s best option is to participate in the WT1 trial. This is a trial through Fred Hutchinson Cancer Research and uses genetically modified T-cells which have a specially designed receptor to bind to the WT1 protein found on 90% of leukemia patients cancer cells. Normally a bone marrow test would be done to confirm expression of the WT1 protein in the cancer cells, because if it is not present, the receptor is useless. However, because Allistaire has not had any detectable disease in her marrow since she relapsed in October, they decided to proceed without this info for now. At the end of this round of chemo, she will have another bone marrow test performed and if there is disease, they can then test for the WT1 protein.
So far 17 people have participated in this trial. Of the people who were in remission going into a bone marrow transplant and remained in remission leading up to getting the modified T-cells, 100% have remained in remission for over a year that they have been followed so far, this in light of a normally high relapse rate post-transplant. There are two people who relapsed after transplant and then got back into remission and then received the modified T-cells. This is the arm of the protocol that Allistaire would fall into. I believe I was told these people are also remaining in remission. The remaining group relapsed after transplant and did not get back into remission and despite having the T-cells are not doing well or have already died. It seems the T-cells work best when there is little to no detectable disease. We will know the state of Allistaire’s disease after we get results from her next set of tests around June 16th. How I pray she remains in remission, but she has been receiving very mild chemo and has gone great lengths of time with little to no defense.
What makes Allistaire unique in this trial, is that, should she be able to get these TCR T-cells, she will be the very first child to do so. I will have to ask again if this is being done anywhere else, but she is certainly the first child ever to have this sort of therapy here (Seattle Children’s/Fred Hutch). There are many kids with ALL (Acute Lymphoblastic Leukemia) who have by now received modified T-cell therapy. But the targets are quite different. In Lymphoblastic leukemia, the cancer is in the B-cell line and CAR (Chimeric Antigen Receptor) therapy is used to destroy the cancer and in doing so, it forever destroys the patients’ B-cell line, requiring life-long transfusions of Immunoglobulin. The first child ever to receive this therapy was a little girl named Emma in April 2012 at CHOP (Children’s Hospital of Philadelphia). She has remained in complete remission since then. Seattle Children’s Research along with the Ben Towne Foundation has provided this therapy to a growing number of children with great success. People are coming from around the world for this treatment. A month ago I met a woman named Solveig from Germany who was here with her son, Nicolas, who was getting CAR-19 T-cell therapy. Allistaire’s cancer (Acute Myeloid Leukemia) is found on the myeloid line – cells that you cannot forever destroy and rely on transfusions for, cells like red blood cells, platelets and granulocytes. Thus the scientists have needed to find another way to attack these cells.
The folks at Fred Hutch have been incredible. I am amazed, honored and humbled by their passionate desire to make a way for Allistaire to participate in this trial. Through conversations with Dr. Bleakley, Dr. Dan Egan (the principal investigator on the trial) and Dr. Phil Greenberg (the head of the lab who has designed this therapy), it is so abundantly evident that they see Allistaire as an individual and they see her as the child that represents the children who are also in desperate need of this therapy, children who have run out of options, children “destined to die of their disease.” They have re-written the protocol to accommodate her, to make way for future children. The original weight requirement was 30kg because of the numerous blood draws required for testing. They worked it out to reduce the limit to 15kg, Allistaire was 17kg at the time they made this change. Additionally, because this weight change equals treating much younger patients, they went through a lengthy, involved process to set up approval to give this therapy at Seattle Children’s. Up to this point, the youngest patients have been in their teens and were treated at The University of Washington where adults are treated. They have worked hard to make a way through for my girl.
On Sunday evening, May 17th, I was delightfully honored to be invited by Julie Guillot to the Premier Chef’s Dinner, a fundraiser for Fred Hutch. As I have mentioned before, Julie and her husband, Jeff, lost their son Zach to a complication of his third transplant for AML. At that time they were helping fund the research that would create T-cells that would give Zach another measure of defense against AML. When Zach died in February 2014, Julie’s zeal and wild fiery passion to bring an end to AML and better treatment options, only intensified. When Allistaire relapsed in October 2014, she invited Allistaire and I to a little party for Dr. Greenberg’s lab to celebrate the $1.7 million dollars Julie and Jeff had helped raise for his research thus far. It was at that time I first met Dr. Greenberg in person and introduced he and his lab staff to Allistaire. Jeff and Julie were the challenge fundraisers for the fundraiser on May 17, 2015, having pledged to match up to $400,000 of money raised that evening. In making this commitment, they were given the privilege to direct where the funds would go. Their whole motivation was to see the immunotherapy through Dr. Greenberg’s lab flourish and accelerate. By the end of the amazing evening, $1,280,000 was raised to accelerate targeted cellular immunotherapy research at Fred Hutch. I had the joy of standing up and representing the hopeful first child to benefit from his research. Dr. Greenberg spoke to me on two different occasions during the evening, each time with multiple hugs initiated by him. You could see the eager joy and hope in his eyes. It was a wondrous thing to stand alongside a man who has dedicated several decades of his life to this research, generous donors, a fellow cancer mom who lost her son – for whom this therapy is coming too late, and I, the mom of a child who is desperate now and who needs this treatment immediately. The full circle was there – scientist, patients, donors.
Doors are opening but still the tension remains high-pitched. There is the illusion of normalcy, there is light-hearted laughter on the surface, but there is a mighty undercurrent, ever threatening to pull Allistaire down, deep into the suffocating dark. First financial approval for the trial was required which was confirmed by Blue Cross Blue Shield of Montana this Wednesday. This allowed the Unrelated Donor Search Committee to initiate their part which is to request Allistaire’s original donor to be contacted and for a request for consent to use remaining donated cells for this trial. At this point, unlike the CAR t-cell trials, the WT1 trial must use bone marrow transplant donor cells. While Allistaire is not in a position to get a transplant at this time, she thankfully does have cells stored at Fred Hutch from her original donor from her transplant in June 2013. Extra cells are stored for two years at no charge and then you have the option to pay to have them stored. This June 18th, will mark two years. I pray this woman can be found quickly, quickly and that her heart will be moved again to give, this time solely of her consent. It feels sort of terrifying to know that Allistaire’s one shot is dependent on a woman on the other side of the world, but then again, she gave once in a much greater way, we so hope she will help make a way through for Allistaire again. If we can gain her consent, processing of the cells will begin and takes approximately a month and a half. Speed is of essence. The T-cell therapy much be coordinated with Allistaire’s chemo schedule. It is my great hope that there may be a way for Allistaire to get these cells prior to needing to begin another round of chemo.
This therapy could be Allistaire’s cure. That would be BEYOND AMAZING!!!! And if not a cure, we pray the T-cells will buy her more time, time for her heart to heal, time for her heart to gain strength to enter the next battle of a second transplant. What’s so wild to me is that Allistaire would be inpatient for ONE day for this therapy. ONE DAY!!!! And this T-cell therapy does not result in the intense cytokine storm response as it does in the CAR T-cell therapy which puts most kids in the ICU for some period of time. No one in the WT1 trial has had to go to the ICU. In fact, Dr. Gardner told me that Allistaire would not be able be eligible for the CAR t-cell therapy because of the extreme dangers it can pose. For the WT1 trial, they would ask her to stick around for a few weeks for some blood draws and observation and then remaining blood tests could be done at home and simply mailed over to Fred Hutch. It all seems too good to be true. What a wondrous world it will be when this is the way cancer treatment is conducted. Can you even imagine?! I must highly, highly recommend the documentary, “The Emperor of All Maladies,” by Ken Burns! It is based on the book of the same name which is also extremely fascinating and worth reading. It is simply thrilling to see how far cancer research and treatment has come and the heightened hope that immunotherapy will change the course of how cancer impacts our lives – for one in every two men and one in every three women who will get cancer at least once in their lives.
I am weary, so utterly weary. But what choice do we have but to walk on? And we do. We walk forward, giving thanks for so much blessing. Sometimes it feels like there being a way through for her is an utter impossibility, but then I am reminded of how many “impossibilities” have come to pass, how the insurmountable has been overcome. My yearning for her life is like a burning fever that never lets up. Every moment is on high-alert, racing through the myriad of questions to try to determine how she is doing, to assess what is going on for her. There are now so many interwoven layers of medical complexity and reality. There is cancer, there is heart failure, there are medications (13 different ones every day – 26 doses), there is being deconditioned by months lived in the cramped confines of the hospital. I see her on the play ground and I watch kids younger than her charge a hill or climb with confidence. She tires quickly, she is fearful. Her legs hurt. Is it cancer on the move? Is it lack of blood getting to muscles? Is it simple fatigue brought on my muscles that have not been asked to do much in so, so long? Is she nauseous? Is it from chemo? Is it from the magnesium she must take because her Lasix makes her waste it, magnesium that causes tumultuous abdominal cramping? All her pain signals are mixed up so that she just finds herself in a frenzy of discomfort, in a frightful maze desperate to get out but with no clear direction.
Leaving the hospital balloons the craving for normal, it makes you think you should be normal, all the standards shift and you see your child not as one among the many other sick kids but among the normal. At the same moment that I am delighting in the warm day and Allistaire playing in the sand, going back to the lake shore to fill her bucket again, I am aware of the dangers in that sand, in that water. I’ve put parafilm on the end of her tubies and tucked them tight into her swim suit. She wears her sun hat and is lathered in sunscreen. Her medications make her more sensitive to the sun, more likely to burn. I’d like to avoid skin cancer. She doesn’t know what to do when the other little girl approaches silently to play with her and share her toys. She is fearful and defensive. My heart sighs knowing how little interaction she’s had with other children, how to navigate such situations. In her cardiology appointment the great nurse, Jason, calls her precocious. Yes, yes, she seems to be quite articulate for a five-year old. There are ways that her deficits are glaring and there are odd ways that she has walked so much further in life than the vast majority of five-year olds. What I know is that I love her dearly, I long to keep her safe, to see her have long life.
I pray to God, I seek to be reminded, imbedded in the truth of His infiniteness. I ask Him to remember that I am finite. I ask Christ to pray for me as He prayed for Peter, that my faith would not fail (Luke 22:31-32). I ask Him to help me to lift my eyes, to take in the long view, to help me in this brutal moment, these series of endless days, in this tedious fight against cancer, in this relentless tumult to see His face throughout all these circumstances. We go to the playground. We look for the first stars at night, our necks craning back. Alllistaire points eagerly at the moon, not framed in the hospital window, but in the vast expanse of the evening sky. We listen for birds and bend our noses to flowers. Our feet follow little paths through marsh land and cat tails, spider webs bright in the afternoon sun. We live, we delight. We go to the hospital again and again into little rooms with blood pressure cuffs and vials of blood that tell of the world within which eyes cannot see. We walk forward through this intertwined life, messy, unclear, wondrous, of such enormous precious value. We give thanks to the Lord and ask for more.























Lyrics above are from J.J. Heller’s song, “Keep You Safe.”
 Cacophony
Cacophony








































































































































































































{kind=link}
{kind=link}