 I know it is redundant, I’ve spoken of it before, but there are just those points about which your mind continues to circle back to, the strange attractor. In the afternoon of Friday, March 11, 2011, a 9.0 magnitude earthquake occurred, centered “about 45 miles east of Tohoku, Japan, at a depth of about 15 miles below the surface.” “The quake occurred as the Earth’s crust ruptured along an area about 250 miles long by 100 miles wide, as tectonic plates slipped more than 18 meters, said Shengzao Chen, a USGS geophysicist.” The result? The earthquake moved the main island of Japan 8 feet to the east, shifted the earth on its axis by an estimated 4 inches and sped up the rotation of the earth by 1.8 microseconds.
I know it is redundant, I’ve spoken of it before, but there are just those points about which your mind continues to circle back to, the strange attractor. In the afternoon of Friday, March 11, 2011, a 9.0 magnitude earthquake occurred, centered “about 45 miles east of Tohoku, Japan, at a depth of about 15 miles below the surface.” “The quake occurred as the Earth’s crust ruptured along an area about 250 miles long by 100 miles wide, as tectonic plates slipped more than 18 meters, said Shengzao Chen, a USGS geophysicist.” The result? The earthquake moved the main island of Japan 8 feet to the east, shifted the earth on its axis by an estimated 4 inches and sped up the rotation of the earth by 1.8 microseconds.
How could such a thing occur, such a radical shift with mind-boggling results? “The temblor (earthquake) completely released centuries of built up stress between the two tectonic plates, a recent study found”
As of yesterday, June 30th, I have lived in Montana, for the second time, for seven years. It has been just over three years since Allistaire died. For the passed six plus months or so, there has been a building tension, a weariness more and more intensified, the layers of pain and loss compressing down. My cry of lament to the Lord has been a pleading to bring this season of loss and sorrow to a close. Can we please be done with this Lord? Can you please bring me into a new season, a season not marked by loss and sorrow and deep loneliness? Many times I have sat across the room with my clients who ask me with plaintive, pleading eyes, the searing question that resonates in my own being, why should I go on with this overwhelming pain? If this is all there is, why can I not just die? The sorrow, the loss, the betrayal, the empty, the radical deep loneliness of feeling cut off, cast out and pervasive, cellular, visceral not-belonging. The small room swells heavy with the questions, honorable questions, questions with the grit and scouring of reality – questions that greet me as I yet again enter an empty house at the end of a long day, as I lay my head on the pillow and wonder what it’s all about, a weariness that lacks the energy to circle round yet again, desperate to find the propulsion that will keep me going.
The rung upon which I cling is the hope that it will not always be this way. I take in their tears, the rage in their voice, the demand for an answer, their moaning that contorts their body as they draw back toward the office wall, an unconscious bodily response of repulsion of the horror that greets them daily. I sit alongside them, my own shoulders weighed down with grief in every direction, the questions pummeling even as I am already on the ground. I hold out my small hands, feeble, cupped as a bowl, and offer to hold hope. Hope for them, hope for myself, that it will not always feel like this, be like this, protecting and nurturing that wee little flame that clings to life, the fervor small and frail that has tasted of something beyond this suffocation.
For six months I daily sat in this chair by the window, studying for my Licensed Clinical Social Worker exam, 21 years since grad school, trying to cram in thousands of new words into a brain that already felt saturated. At times I wanted to scream out that my brain had already been asked too much, had finally learned the language of medicine and cancer. Once foreign and new to me, I learned to speak fluently – febrile, nadir, kinase, cytokine storm, monoclonal antibody, gemtuzumab ozogamicin, bortizomib, mitozantrone, ejection fraction, LFTs, vancomycin-resistant enterococcus, and my all time favorites – the “vincristine push” and Entresto – no, not “Ernesto” – it’s heart drug, not a Hispanic man.
And now I was asking this same brain, who had already learned this language of oncology, cardiology, immunology, pulmonology and nephrology, because the actual life of my child was on the line if I failed to master it, to yet again sit with a gun to my head. Again it felt like a life was on the line – this time mine. Learn this language of psychology and therapy…or else. So I memorized the 12 criteria for catatonia which is easily recalled by the phrase “Stupid Cat Flexed and Grimaced at the Posterior of an Agitated Man who Steered his Mutts, Echolalia and Echopraxia, by their Necks” which is supposed to help you remember Stupor, Catalepsy, Flexing, Grimacing, Posturing, Agitation, Mannerisms, Stereotypy, Mutism, Echolalia, Echopraxia and Negativism – easy peasy lemon squeezy as Allistaire would say. Lists of typical and atypical antipsychotic drug names got smashed in there along with SSRIs, MAOs and SSNRIs. Now I can tell you all about Erik Erickson’s stages of development, Piaget’s stages of cognitive development, and Kolberg’s theoretical stages of moral development. I can tell you how many times a week over what period of time you have to binge eat to qualify for binge-eating disorder, how many days in a row you must have exhibited “expansive mood” to qualify for having bi-polar I versus bi-polar 2 and how to differentiate between schizophrenia and schizoaffective disorder. You know, your mom may just be the way she is because she’s stuck in the anal stage according to Freud. On and on it goes, all the while I feel the cold pressure of the gun’s muzzle against my cranium frantic to cram in more and deliver it in sensible manner during that four hour exam during which I am not even allowed to drink water.
The winter has been relentless, even absurdly reaching 32 degrees and snowing on June 20th. The relentlessness of the winter has paralleled this domination of sorrow and gun against my head sufficiently propelling me to not relent, to press on, desperate to be on the other side of it all. And as the exam of May 29th approached and my studying seemed to reach its culmination, I found myself in a sort of quiet lull, and eerie time between times. The hair raised on the back of my neck and I felt my throat clamped tight. What is this, I asked with voice low and cautious.
It was as though in all my rush and fury, blurring of tears and frantic ceaseless action, I had unknowingly come to the edge, to the end of the horizon. Suddenly I realized I had no idea what lay on the other side. Just as I had focused all my energy and courage to get through my first pregnancy and just have my child safely delivered, I found the looming question, “now what?” For eight years I have lived with and become accustomed to the terror of life-or-death. The black form of the reaper has ever stood in the corner of the room, it’s heavy dark presence sucking in any light that dares come into its orbit, always in my periphery. So intimately familiar with impending storm that ravages and destroys, with the metallic taste of blood and salt while thrashing out in the dark waves, I found myself bending forward, eyes squinting, what now? The bottom has dropped out time and time again. The potential for loss remains. Turns out there is no quota for suffering, there may be and likely is more to come. My Papa Murphy will be 96 years old this September. “Forty-plus possible more years of this?” my heart cried. Oh God, oh God. Must I go on if this is all there is? Let me be done God.
With only seconds remaining, I pushed the button on the computer to say I had completed the exam. My hands shook, my stomach cramped and heat stung the back of my neck. Passed. And just like that, the efforts of the past two and a half years since my husband walked out of our life, leaving me reeling, grasping for some path toward financial stability, it was done. On June 6th I received word from the Montana Board of Behavioral Health that I had earned my Clinical Social Work License, a credential that means little or nothing to most who hear it, but is the pivot point for me financially and professionally, opening doors before me.
You see, I never wanted to be a therapist, it had never even occurred to me. What I knew from the time I was an adolescent, is that employment is a trade, an exchange of money for your life. Literally, I carve out these hours here and these hours there, like scrapes of my skin, flints of my bone, ounces of blood and I hand them over. In return? I get money. It’s all a bit sickening really, gross but necessary. So I determined that such an exchange was not enough for me. No, there must be more. So I set out to look for work that would yield more than money. Passing through medicine I landed on social work. I have memorized the six core social work values, honestly having forgotten their specifics from schooling so long ago. They are Service, Social Justice, Dignity and Worth of the Individual, the Importance of Human Relationships, Competency and Integrity. They are summed up in love and laying down your life for all – every single one of us humans, bearing the resplendent, other-worldly, image of the living God. And more, there is a fierceness in that love that stands in shield of those whose very lives and well-being threaten to be crushed by all the brokenness of this world. It seems that God, incarnate in Christ Jesus, was the very first social worker, who declared worth and value and treasuring of those often disregarded, dismissed, passed-by, reviled – the poor, the orphan, the widow, the barren, the sick, the imprisoned, the foreigner, the not-belonging.
I have felt the sting of these. For me there is not even a word. I am a mother whose child is dead. I am on the outside of my own native tongue which does not even offer me a place, a standing. I offered to carpool to a work meeting the other day, when my co-worker gawked at my Suburban, asking me why I drive such a thing. The question of why one individual would drive a vehicle clearly made for more, inherent. I stuttered and stumbled, trying to explain that it once made sense though little now does. I remember learning long division in elementary school. How satisfying it was when the little number fit so perfectly into the big one and how agitating a “remainder,” as though no one knew what to do with this extraneous left over bit, the little hunk of dough left after cutting out biscuits, fit only to be thrown away. I feel the sting of being a remainder, a family of one-point-five. I don’t fit anywhere and no one really knows what to do with me, other than to remember me on major holidays and invite me to their gatherings, never apparently being worth including of my own accord in an ordinary week.
My sorrows do not make it possible for me to know what it is to have as your first memory being taken from your mother in a police car with stuffed animals in the back seat, daily gasping at the blunt force trauma ever fresh that somehow you were not wanted, not deemed worth keeping and can only guess that you must have been too ugly a baby. I cannot taste on my tongue the cigarette smell of your father’s mouth pressed on your little girl lips and his hand putting your hand on his crotch. I cannot imagine that Disney’s Lion King is synonymous with remembering the panties you wore as you were raped in that bed, perpetrator on one side, your little sister on the other. How can I begin to imagine the impossible decision before you to keep that baby or not, to consider a second abortion when you daily struggle just to survive in your own skin, unfathomable that you have the capacity to care for this new innocent so frail life when you have asked in agony again and again how you are to live out each day.
My own path does not allow me to know what it is to have walked that of another, but it has led me to sit in community with those who also ask weighty questions in the darkness, hearing our voices consumed by the black with no seeming answer in replay, no clear way to bind up the oozing, festering of lacerations, that even mere air passing over causes a wincing recoil.
As I moved the cursor and it hovered over the word “complete,” I shook from head to toe. And with the appearing of the word, “passed,” the tears came hot and unrelenting for twenty minutes or more, I incapable of stopping them, trying to force a smile so the test proctor would not be too concerned as he approached me with forehead knotted. “I’m fine, I passed,” I weakly uttered. To the back bathroom stall out of the testing center I fled, and sat there on the toilet, face in hands, crying and shaking. All I could say over and over was, “thank you God, thank you God, thank you.” How many times have I walked and stumbled, my hand shooting out to regain balance, tears blurring my sight, muscles weary and mechanical, a mantra simply to walk through the next open door? How many times have I stood on the other side of the door, mouth gaping, shaking my head in awe – He did it again, my God went before me. Every single time feels like a miracle, because it is.
That most recent door of becoming an LCSW, is one more way to live out the absurd privilege that God has granted me. Who am I to have been born an American in the 21st Century in a white girl body to English speaking parents who loved me and raised me in a stability that has yielded 50 years of their marriage to one another and financial means to send me to college and grad school and a brain that works decently well and a personality that has helped shape this path? Do I get to take credit? Nope, I sure don’t. But I am compelled to live out the belief that this privilege calls me to wield it in a way that cares for the lives of others, many of whom have had much more difficult, often brutal, starting points. Hence I am a social work and mighty proud of it, and God has seen fit through heart, personality, education, experience, the guidance and mentoring of those wiser and further down the road than myself, and little pieces of paper with letters like LCSW, to hone my craft of care bit by bit to more effectively love.
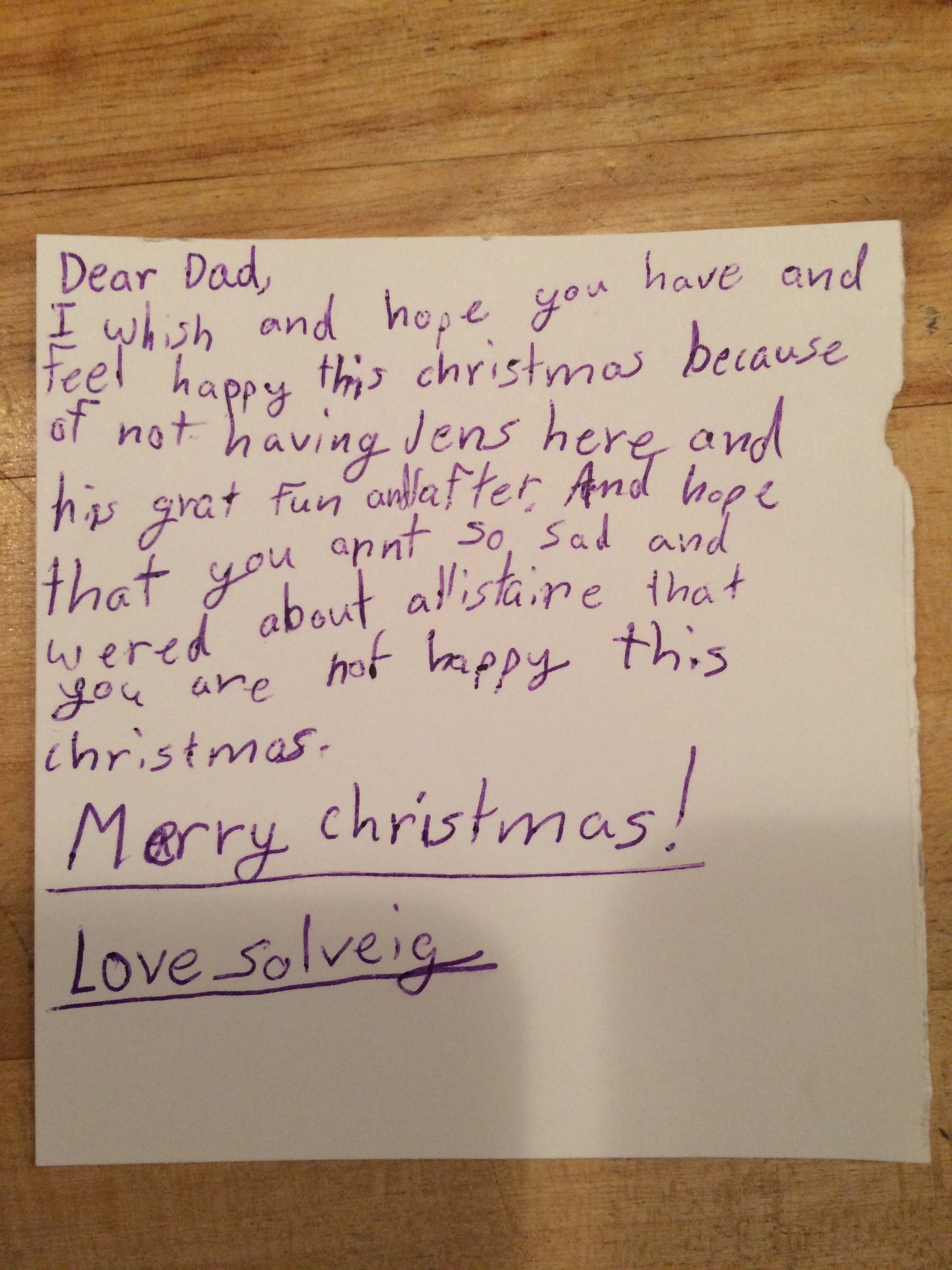
Having the fantastic relief and joy of passing my exam and earning my license, gushing in came the repeated refrain of “now what” tied tight to the longing to be done with this season. There seemed to arise a pulse of my flesh which pressed out the words, “I am ready to set down this grief.” I don’t know that one can “will” the Lord into doing what you ask, but through flex of arm and movement of leg, and scanning of eyes, I have set about in this past month to purge my home of all that belonged to a life that once was and is no more. At long last I have determined to live in the present. Turns out to be a radically difficult feat for me, but into the trash I tossed the little purple piggy bank I painted with Allistaire’s name. The great green monstrosity of my wedding album, the dog brush whose matted hair has sat for five or six years unmoving, the pack-n-play and board books, the little shovel and rake all went sailing into the trash. One of my clients works at the receiving door of Goodwill and just shakes his head as Sunday after Sunday I pull up with a car load full to the brim. I’ve sorted bags and bags of cards received after Allistaire’s death, countless drawings by kids who said they loved Allistaire and prayed for her every night with crayola drawings and spelling challenging to decipher. I sat for a whole half a day on the carpet with a ring of papers surrounding me – echocardiograms, bone marrow biopsies, flow cytometry and chimerisms, labs and bills. There were pages scrawled with notes in my own hand trying to make sense of it all, trying desperately to comprehend the words the doctors were telling me – to somehow use my rational, analytical pre-frontal cortex to make a way through while my limbic system was screaming in agony, a frenzied blur of misfired direction to survive – fight? flee? stuck like a frozen version of myself having no clue which way to turn. I whittled it all down to a few inches thick of paper that now sits neatly in a little plastic bin with a green handle.
I have two full outside garage cans worth of papers to recycle. Over half of my books have been swept off the shelves, many of which came from a time in my life in which I was steeped in a world that sought to debate nuances of theology for which I now have little to no energy. It seems King Solomon’s words in Ecclesiastes still ring true, “I saw all that God has done. No one can comprehend what goes on under the sun. Despite all their efforts to search it out, no one can discover the meaning. Even if the wise claim they know, they cannot clearly comprehend it.” Even as I write this I laugh, knowing there are those who will feel compelled to debate me on this bit of scripture. God’s word absolutely matters, and these days I am easing back into His grace knowing there’s a lot I won’t get “right” but setting my intention to live out a reflection of his love. Do I join my client in going to her abortion? Do I leave her alone in the dark of her misery and agony so as to ensure that my “stand for truth” will not be muddied? Can I love and value the life of the unborn and the life of my patient too – at the same time? I’m sure gonna try and I trust God’s grace can handle it. A tangent I know…
I sorted through all the photo albums, having to throw out the evidence of an entire life which cannot go forward into the next. Her closet is finally empty, having at last folded up the Disney night gown in which she loved to twirl. At long last, I went to the funeral home and had them divide Allistaire’s ashes into the two blue urns, one for me and one for her dad. I asked with cracking voice if I could make a strange request, realizing as the words came out of my mouth that the funeral director had probably heard it all. “Can you set aside a few bits of her bone?” I could see them white in the bag of grey ashes, a bag weighing only 2.25 pounds. “The remains” – language the funeral director kept using in reference to my baby girl who weighed 8 pounds 3 ounces when she was born. How could I explain that somehow I needed to have those bits of bone, the only remains of molecule connected to molecule to create the flesh that had begun in my womb. How could I explain that these bones were the birth place of her death, a marrow that spewed out rot and broken when it should only have been the means of life. What would I do with these bits of bone, I did not and do not know, only that while somehow I can imagine spreading her ashes in the wind or water, I must hold onto some fragment of her flesh.
And as the spaces empty and I contrive how to get rid of more, there is a lightening, there is getting out from under a pressing weight. Just over a week ago, I sat once again on a Saturday morning, drinking my coffee, staring out the window watching the aspen leaves shudder and quake and glitter in the morning sun. I sat with a little book with purple binding on my lap, and honestly a grumpy assumption I was about to dive into another cheesy Christian women’s devotional that would make me want to puke and dump it too into the trash. But Tara had heard this woman speak and mailed me this book, thinking of me. I ought to at least take a look at it.
I haven’t the time at present nor energy to begin to describe what happened next. I can only say that just as after years of building tension, such a cataclysmic shift occurred on the earth that the island of Japan moved and the earth tilted on its axis, so in a twinkling of an eye did the Lord shift my heart. Years of build up proceeded this moment, but it manifested in the time it took to read three pages. The Lord gave me a taste for what may lay down the road, off in the distance there is the shimmer on the horizon of a place worth journeying to, a path worth treading, a way out of the darkness that demands an answer for the point of my existence. The refrain that rose spoke, “perhaps endeavoring to alleviate some of the pain of others is reason sufficient to endure my own agony.” Funny, sounds like my all time favorite verse – in Hebrews it tells of a man who though he huddled in agony in a garden, asking repeatedly for the Lord to let this cup pass, He concluded that “for the joy set before Him, He, Jesus Christ, would endure.”
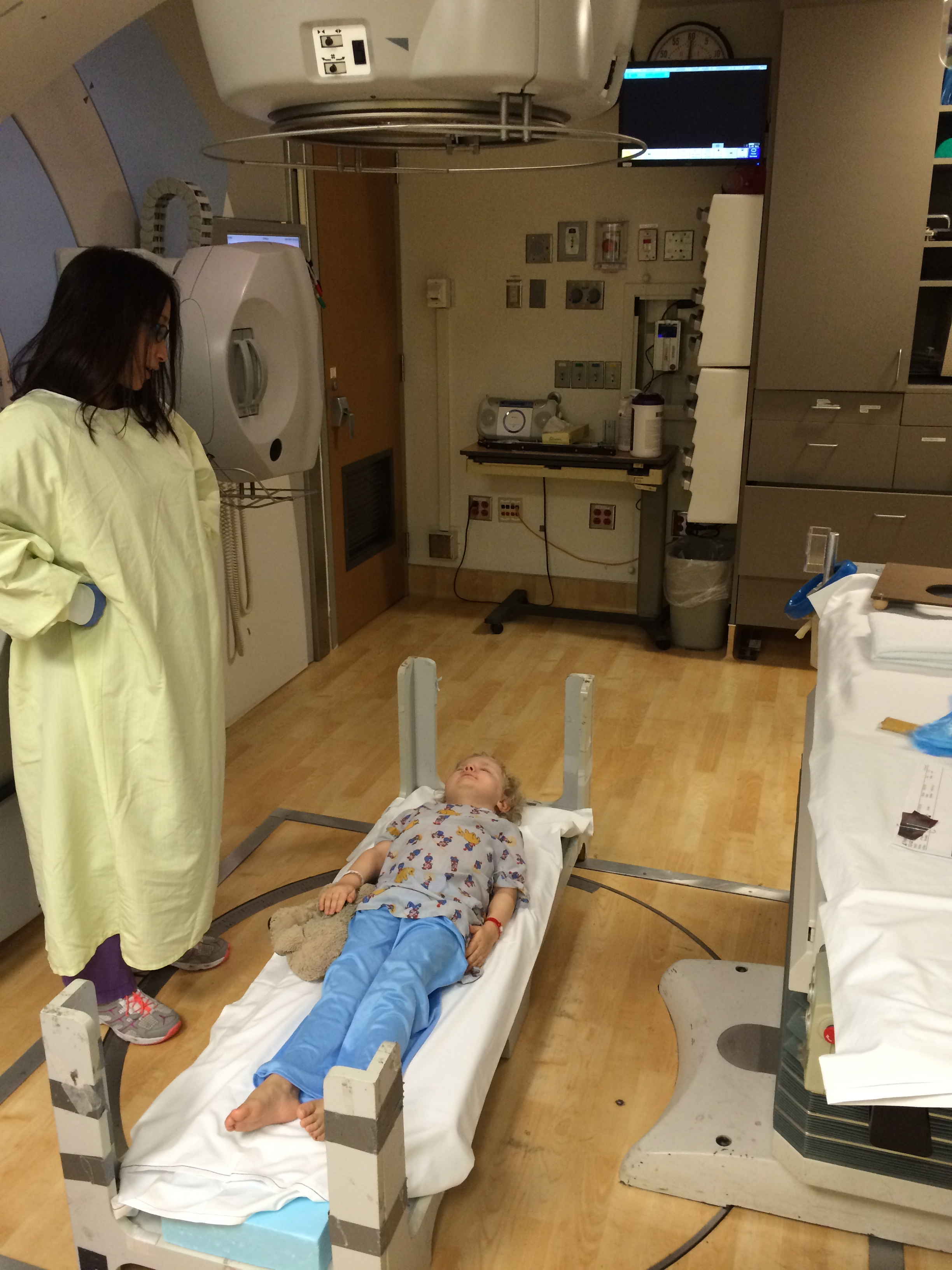
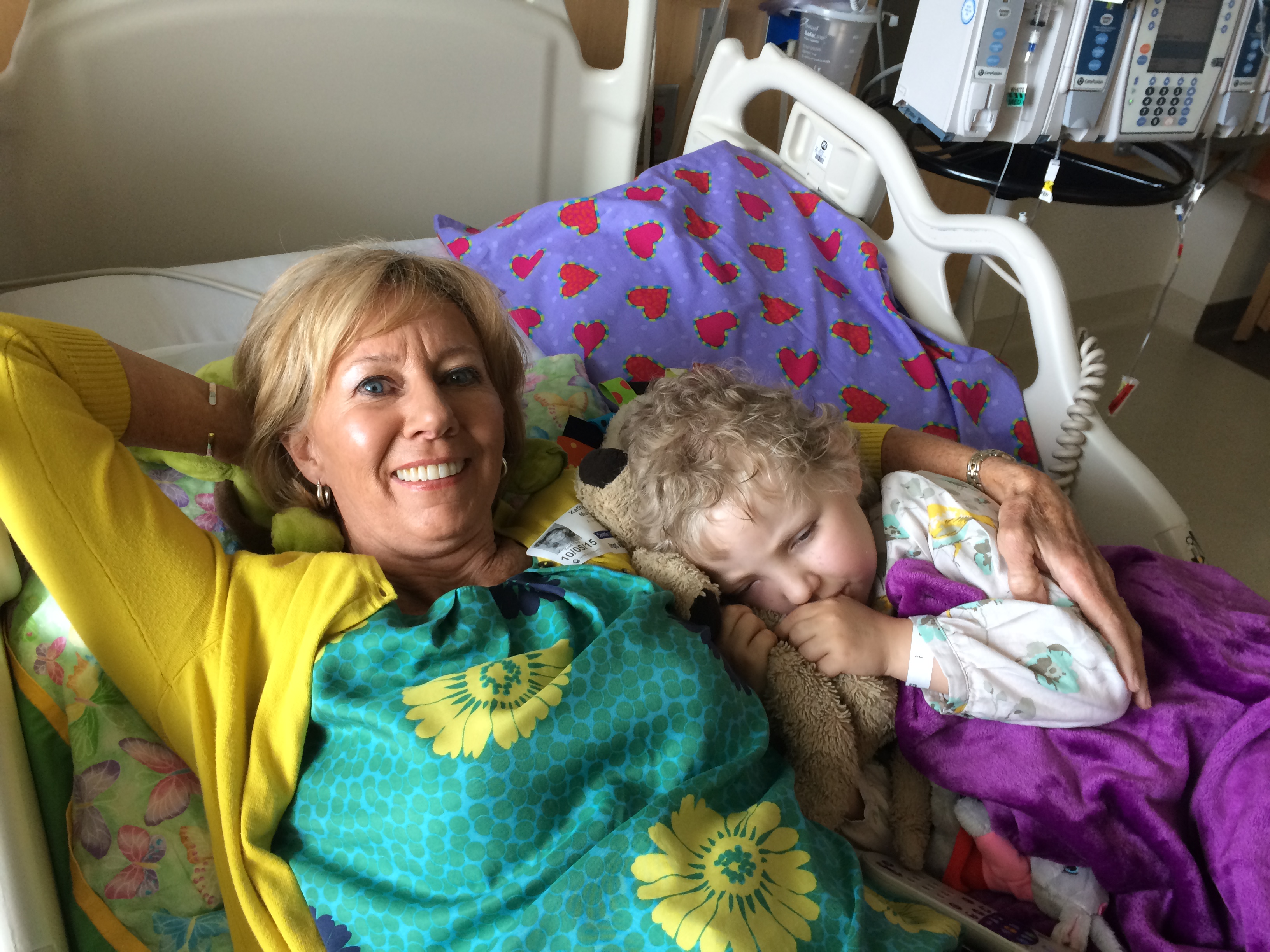
To be honest, I’m tired and hungry and have the lawn to mow and the bathrooms to clean in anticipation of my parents visit. This is one rare day off from work I’ve taken and I didn’t want to spend hours of it writing here, and certainly had not planned to do so. Yet in my sorting I came across a series of pictures, pictures I took to show in a way no words ever can, what cancer IS – the bulging pressure of insane dividing cells that will not stop but press out the eye of your child so you can hardly bare to look at the ghastly white of eye that you should never see, nor the black blood that drains out of her nose because the cancer cells are filling her sinuses and purple of bruise along her cheek or the call for more pain meds because your little sweets is suffering and now matter your heart, you can’t make it stop.
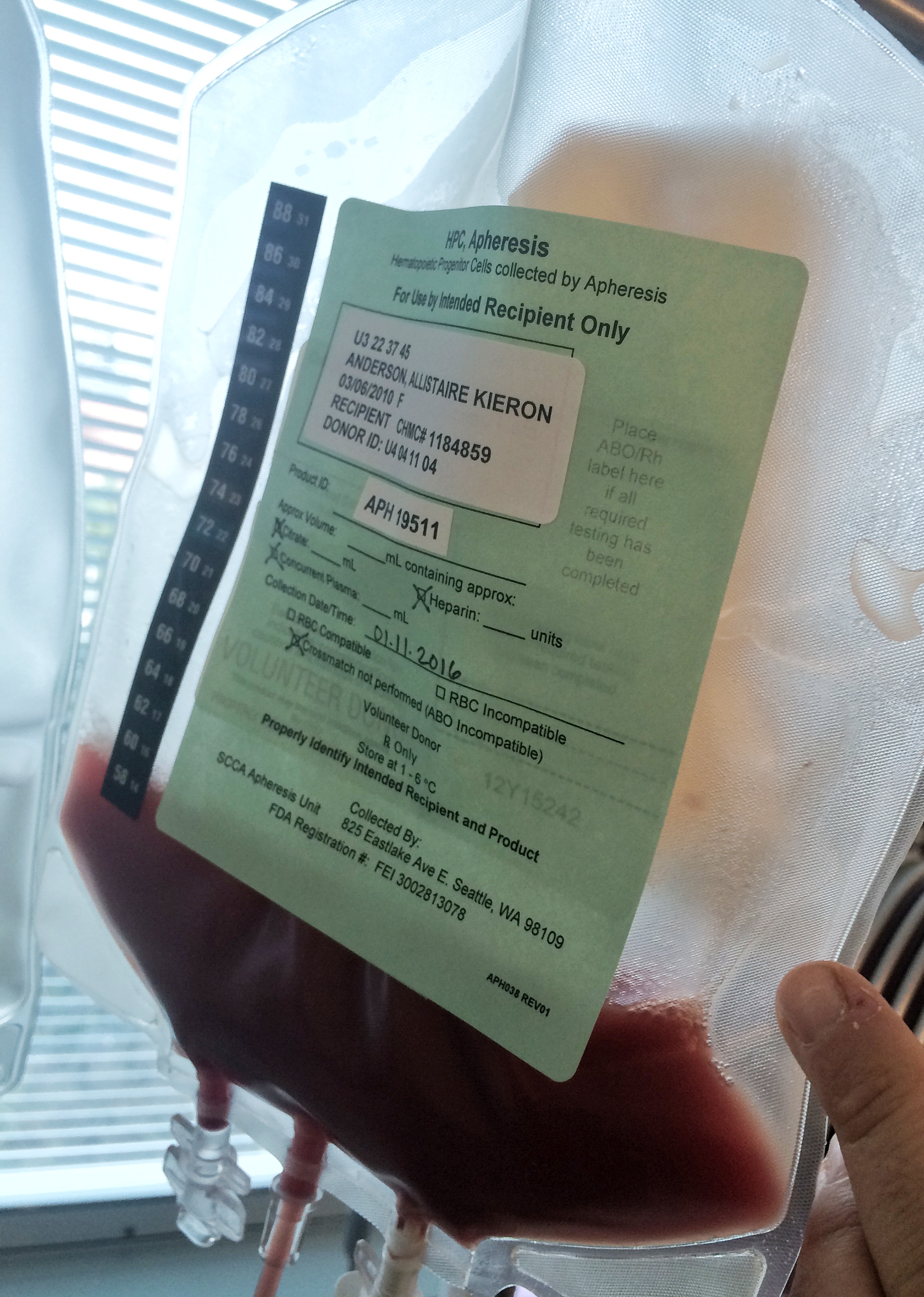
I have no energy to go back through this post and correct the inevitable spelling and grammatical errors. The truth is that in just over one month, I will for the seventh time, swing my leg over the saddle of my orange bike and pedal my way through miles of Seattle asphalt in a feeble human attempt to slow, and dare we hope – stop, the onslaught of cancer. I am again asking you to consider helping support cancer research at Fred Hutchinson Cancer Research Center. The series of pictures show not the progression ,but rather, the retreat of Allistaire’s cancer in the face of this beautiful monoclonal anti-body drug conjugate, Mylotarg, sometimes known as Gemtuzumab ozogamicin. Dr. Irv Bernstein’s lab at Fred Hutch developed this drug years before my little girl would be in desperate need of its weaponry. Allistaire is dead and her cancer overtook her in the span of two weeks with a white cell count of over 256,000 – 14,000 being about normal. Her blood was sludge from being packed with acute myeloid cancer cells. I watched my child’s grey mouth move like a dying fish on the shore and I will have to live with that image and the sounds that accompanied it. I will have to live with the letter from the boy who writes to tell me their horse just had a baby they named after Allistaire – Sapphire Rainbow Sparkle Jewel, instead of seeing that bright spark of a girl continue to burst forth extravagantly in this life.
Allistaire’s cancer cells are stored at Fred Hutch in Dr. Soheil Meschinchi’s lab which holds the largest repository of pediatric AML cells in the world. I will not forget the tears of this brilliant man over the loss of this seemingly insignificant six year old girl whose life cost $10 million to try and save. I have said it before and I will say it again, until cancer is cured, Obliteride is no more or I am dead, I will continue to exert my small human efforts to try to alleviate some of this human suffering. What more is the worth of my life than this? What better task to put my hand to, to give my money to, to exchange the minutes and hours of my life for than to call out to the Lord for life again and again and again.
Every where I turn there is brokenness and loss and rot in staggering array. Ever where I turn I can see if I am looking, that life presses on, that the light overcomes the darkness, that the winter ends, that out of the dark grime of dirt comes resurrection. I cup my hands in this feeble bowl and I hold hope. I am looking for redemption and I stand boldly in the throne room of grace asking the Lord to show His goodness in the land of the living, because He has invited me to do so, on the basis of my magnificent Jesus who sits on the throne.
To exchange a bit of your life for the well-being of others by financially supporting cancer research at Fred Hutch, support me in Obliteride by giving HERE
To read more about the crazy amazing doctors and research at Fred Hutch that directly relates to my girl who was a whole lot more than med rec number 1184859, check THIS out 🙂
For any arriving late to this story, or for those who wanted to make it to Allistaire’s service but couldn’t, here’s a link to that service three years ago in which I attempt to articulate what transpired. Plus, I guess I should have provided this link long ago – oops.





















































































































































































































































{kind=link}
{kind=link}