 Delayed Gratification. Joy Set Before Me.
Delayed Gratification. Joy Set Before Me.
You can endure a lot…if, if you see a glimmer of light. If you can grasp onto that shred of hope. But if it’s all for not, if nothing will come of all your straining, all your loss and sacrifice, it’s ever so much harder to press forward.
But…you catch that glimpse…you sense before you that the light is coming and it invigorates you to lean into the endeavors before you.
I don’t know if Allistaire will make it out of this alive or not. There is so much good I can easily imagine if she lives. There is also good I can imagine if she dies. If she dies, I pass over that line. I enter a territory I have never yet had to tread. If she dies, I will dwell there, with them, with Beth, Merle, Rachel, Julie, Devon, Ryan, Darliss, Janett, Shannon, Susan, April…I will share in their company and that would be good and I would have an understanding that at this point is only imaginings. I cannot let go of my sweets but it hurts my heart to not be able to draw yet closer to them in their places of pain and hope.
For now, we are here, here in the dark but with a glimmer. For me the glimmer began with remembering the statement that, “I would be flabbergasted if your insurance approved this transplant.” This was voiced by a woman who has been integral to coordinating all the details of transplants for years. And you know what, Blue Cross Blue Shield of Montana has approved Allistaire’s transplant. Flabbergasted has happened and it was a sweet, tangible reminder that the “unlikely,” has happened so many times for Allistaire – good and bad. What shouldn’t have been, has. So if the doctors say she probably won’t recover the needed heart function, well, they could be right, but they might not. Flabbergasted can happen. It is a reminder that God will do what HE will. There is SO much to tell, so much in fact that I’m sure I will fail to get it all down.
When did the shift begin? On February 15th Allistaire finally showed evidence of her bone marrow recovering after 38 days at zero. Then there was a solid week of serious pain as her white blood cells flooded her gut and got to work on healing. Sometime in the few days preceding our especially difficult care conference, as her ANC continued upward, her pain began to subside to the point that she now needs only one dose of pain meds every several days, if at all. On the day of the care conference something wondrous happened. Her BNP (Brain Natriuretic Peptide), dropped below the terrifying lab value of greater than 5000. This has been its approximate path: Over 5000, 3800, 3200, 4000, 2600, 1400, 972, 1040, 1320, 1090, 2350, 552, 1100, 749, 1070. The big blip back up to 2350 was most likely due to getting blood the day before on her birthday. A transfusion of blood resulted in a big increase in fluids and blood is a very heavy fluid so while the heart loves blood, the big extra dose caused a bit of distress in that narrow window. I cannot convey to you how glorious it is to have that wretched number dropping! I have no idea if it’ll keep going or if it will settle at some point.
Another development is Allistaire’s overall activity and joy level. The girl is coming back to herself! I remember trying to get Allistaire out of her bed after a week in the PICU to have her walk to the door of her room – it was such a great and painful effort. In reflecting back to the days after Allistaire’s transplant and being in bed so much, I knew the sooner we could get her walking again the better. The scope of my abilities to directly help Allistaire through all of this are so limited, but I knew I could help her get moving. So what began as one walk a day from the bed to the door turned into a lap from bed to couch to door and back to bed, three times a day. We kept increasing the distance and the frequency. Thankfully, the Infectious Disease doctors approved the same activity plan she had up on the Cancer Unit which meant we could finally leave the room as it was getting absurd to try to make progress within the confines of her small room. We are now up to a lap around the PICU and Cardiac ICU five times a day. That is equivalent to a half mile a day. She giggles now. She jokes with the doctors and nurses. She plays around in her bed and kicks and seems to have no limitation on her movement.
Last week Dr. Yuk Law, head of the Heart Failure team, was our attending cardiologist. One of my greatest joys has been seeing him watch Allistaire with a look of disbelief on his face. My impression of him, which has been supported by that of others, is that he is a very even keel man. As he watched Allistaire frolic in her bed, he pointed out that she was moving a lot. “Well, yeah,” I thought,”that’s Allistaire you’re looking at.” I then went on to tell him about her progress in walking around the Unit. With a look of surprise, he asked me to clarify that she was, what, out of her room, walking around? Yes, yes, around the unit five times a day, I reiterated. You see, she is literally the only person in the whole ICU who is walking around. He wanted to know if she got out of breath. “Not even a hint of out of breath.” He said he was astonished. He watched to see her as she finished a lap to verify my report. With a dropping BNP and such incredible physical activity, he discussed the possibility of trying to wean her Milrinone, but he wanted to wait for Monday’s echocardiogram.
Flabbergasted. Astonished.
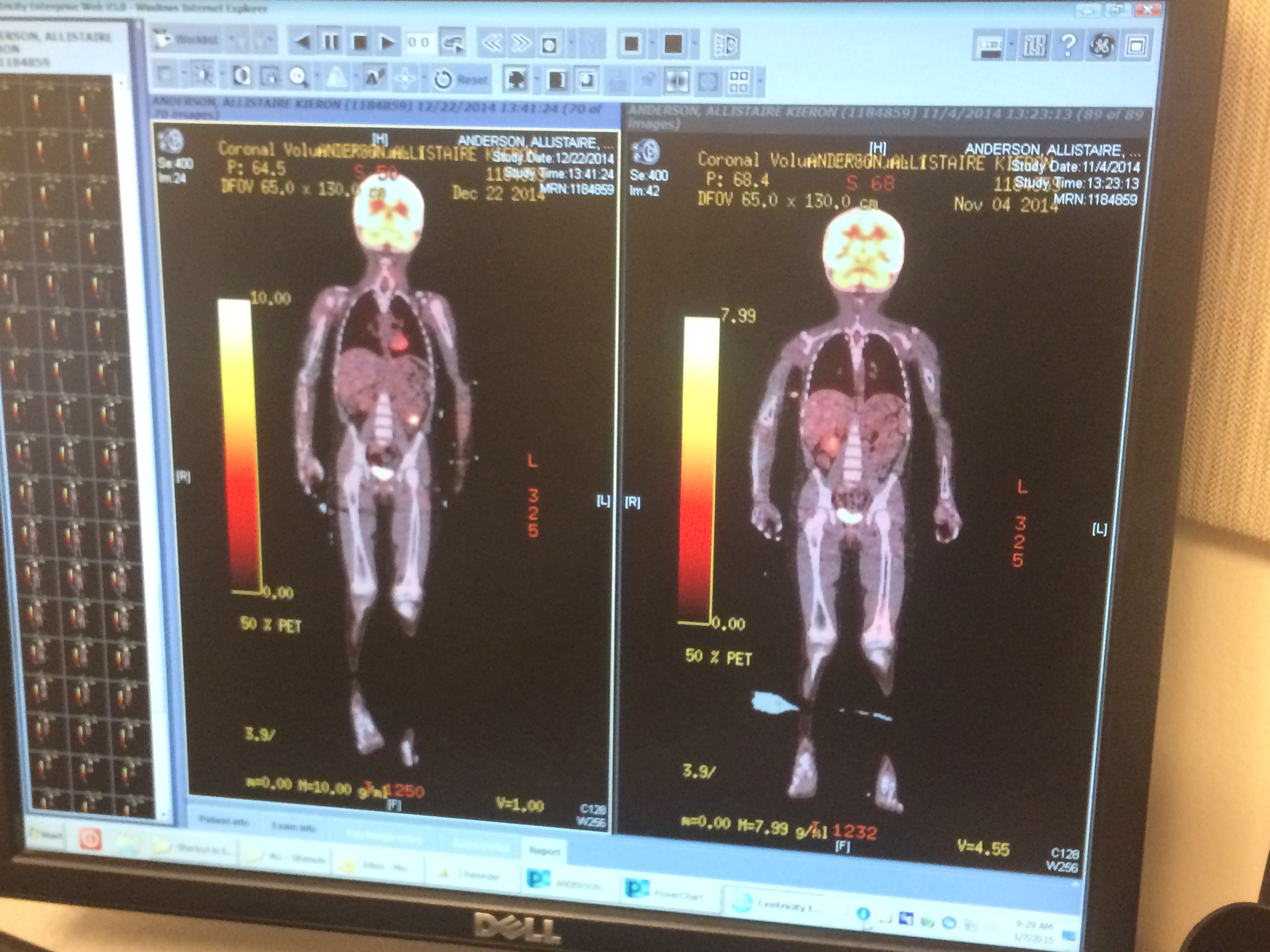
On Thursday, March 5th, two weeks after her last discouraging CT, Allistaire had another. This CT would look for fungus in the sinuses and chest with the hopes that if it were not there, we could stop the Micafungin, which is a very broad spectrum IV anti-fungal, and return the prophylactic, Fluconazole. They would also look at her gut to see the state of Typhlitus. If she was all healed up, they could finally end over 50 days of broad spectrum antibiotics. The CT showed that the sinuses were completely normal and clear. Moving down to her chest, it says the “lungs are clear. Previously noted predominantly sub pleural groundglass opacity and consolidation has resolved. The proximal airways are patent. No pneumothorax or pleural effusion.” Previously noted small right pleural effusion from 2/20/15 has resolved.” Did you get that? Things look normal. Issues have resolved!
It goes on: No enlarged lymph nodes (a common place for her cancer). The liver, spleen, gallbladder, biliary tree, pancreas, adrenals, kidneys and bladder are normal. No pathologic mass identified. Previously noted multifocal bowel wall thickening involving the colon and rectum has resolved. The bowel is now normal. The appendix is normal. What sweet relief! Her whole gut has totally healed, there is no fungus and you know what, even previous evidences of heart failure in her lungs and liver were not mentioned because they are not there! I was so elated! This also meant two more IV meds are done. Over the preceding week, we had begun to transfer IV meds to be given by mouth as she could handle it. As of today the only IV meds Allistaire is on is Milrinone and Lasix. Of course, she takes a total of 20 doses of meds by mouth each day, but a number of these are just preventative.
The other big development is that Allistaire has begun to eat. I joyously charged into Pagliacci Pizza last Monday evening to declare that my girl, who had not eaten in nearly 60 days, wanted cheese pizza and lemon San Pelligrino. She ate with a zeal of old. Then she threw it all up. Too much too fast. Over the last week she’s struggled with nausea but continued to have an appetite, even requesting a hotdog the other morning before 8am. Tonight’s request is chicken quesadilla, rice and chips from Chipoltle. The nutritionist was able to reduce the calories in her TPN (IV nutrition) and get rid of her lipids all together. Over the weekend, Dr. Law decided to have the team completely cut the TPN given that oral fluids have less of an effect on the heart than do IV fluids. I won’t deny that I was surprised and frustrated by this rapid adjustment. Getting Allistaire to eat is a time-consuming and often very challenging, stressful process, especially when it all ends up in being thrown up. Nothing is more defeating. A typical meal requires 2-3 hours of tedious intermittent bites and prompts to drink. By last Friday she was probably taking about 500 calories in a day with a total daily goal of 1,200 calories. So much of it is hoping Allistaire won’t be over nauseous (she is on anti-nausea meds she gets every 6 hours) and strategy – what will give her the most calories that she can also keep down. (By the way, this is not a request for input on this matter. Believe me, I’ve had countless conversations, and innumerable attempts at a variety of options. We are three plus years into this food battle and I admit, advice at this point is not welcomed.) Yesterday the girl got 1,300 calories in. I was amazed!
Today we’ve had to make a few food adjustments due to an “acute kidney injury.” As a result of all the Lasix, which pull off fluids and are thus quite hard on the kidneys long-term, and an electrolyte imbalance, her BUN (Blood Urea Nitrogen), Creatinine and potassium levels have crept up and were quite a bit too high today. Because they monitor all of these levels daily, the doctors are able to catch issues early and make adjustments. A number of meds were held this morning that impact potassium levels and fluid load. Also, I am not giving her milk or orange juice today, both of which are high in potassium. They retested labs this afternoon and thankfully her numbers have trended down now nicely. Most likely she can resume her regular meds tomorrow.
The issue with her kidney’s also prompted a hold on the planned wean of Milrinone, originally set to begin today. Allistaire had her echocardiogram on Monday. It was a bit deflating. Dr. Hong, the attending cardiologist this week, said that while the EF (Ejection Fraction) is up to 21% from 11%, she says her heart looks about the same. We had a lengthy conversation which included looking on the computer at her echo from back in December when her EF was 65%. Of course there was a marked difference. Dr. Hong seemed cautious to not be too optimistic and over-promise. This was where we had a bit of tension. I’m not looking for grand results in two weeks time. I’m looking for a shred of hope that shows she is going in the right direction. I’m looking to take stock of every victory no matter how small. I know it is no guarantee of what will come, but I have to live out these days and I need that fuel of hope to keep me going. Dr. Hong did say that her right ventricle, which had looked fine until the last echo two weeks ago, had improved, as had the function of the mitral valve. They haven’t recovered fully but they are better than they were before. Hopefully this recovery will in turn aid the recovery of the left ventricle. The cardiologists will meet today to discuss med changes including the possible addition of another med and the likely wean of Milrinone, set to begin tomorrow.
I have never felt so weary, so utterly tired. The planned wean of Milrinone will be incredibly slow this time. Last time they weaned from .5 to zero in a week. This time they plan to wean .1 per week, starting at .75 which means a seven and a half week wean to zero, five times slower than before. This is wise because we all want her body to have the very best shot at successfully coming off. Yet, as I calculate out the very, very best scenario it would be three more months until transplant, which assumes the ability to keep her cancer in remission, a successful wean and sufficiently improved cardiac function. This is a lot to assume. Nevertheless, if you add these three months to the 100 days post transplant one is required to stay in Seattle for, we’re looking at a minimum of six more months. I’m packing up my wool sweaters to send home with my mother-in-law, JoMarie. But I’m wondering if the seasons will turn again and again with us still here and I may need to wear them again in this place. Daunting. So very daunting.
Friday was Allistaire’s 5th birthday. It was a crazy, whirlwind of a day, fun and emotional. The point of celebrating a birthday is to remember back to that day your beloved came into this world and to express thanks for each year since. I could never have imagined when Allistaire was born that this fight against cancer would exist, much less so consume her days. Four out of five birthdays have either been in the hospital or under the shadow of treatment. We did nothing for her second birthday but be glad to be home after leaving the hospital the night before at 11:30pm when her last dose of chemo for that round had been given. Her third birthday was spent in the hospital soon after her first relapse, just the two of us. Her fourth birthday was a grand event at home, only two days after she had her Hickman line removed at Seattle Children’s marking the end of treatment but with the looming fear and wonder of what the coming year would hold. For me Friday was a day to be in both wonder and in sorrow. It is wondrous to me that her life has been extended over and over and she is here with us for another birthday. And my heart is heavy with grief that her little girl years have been so constrained. I think of the lives of other little girls and the contrast is so stark – like a sudden punch in the stomach. I am so keenly aware of the fact that this could be her last birthday, that her life ever hangs in the balance. Tears threatened throughout the day.
I also nearly cried as we walked into her room that afternoon. A sweet woman, Libby, from Soul Illuminations, had volunteered to come and take photos of us so we had headed down the hall to the Quiet Room where the visuals are better. When we came back to the room, the bed had been shoved to the far wall and the room was full of joyful faces eager to celebrate Allistaire and see her delight. Sarah from PT (Physical Therapy) came with her parachute and a group was bouncing a beach ball a top the parachute. There was music and clowns and cakes and too many presents and just a whole lot of love. Again I had to hold back the tears – that she would be so loved, so celebrated, that so much planning by the hospital staff would go into making this day special for her, well, it was overwhelming in such a beautiful way. And it was a special joy to have Solveig and JoMarie surprise her for her birthday. Ah, two sisters giggling. There is nothing better, nothing.
When Allistaire was two weeks old I took her to see Caroline, her great-grandmother who was in a nursing home. We arrived to find Caroline in her group time with fellow Alzheimer’s patients. Two of the women asked how old Allistaire was. I told them, “Two weeks.” “Wow, just two weeks,” they exclaimed with ooos and sweet faces of cherishing delight. A minute later they would ask the same question, which yielded the exact same level of surprise and delight. This went on and on. Same question. Same answer. Same response. It was comical in one sense, but I realized that this question yielded a wonderful answer. What about when these same women asked about their husbands who had likely passed away. They had to meet the news of their beloveds’ death over and over, with the same shock and sorrow. It’s not quite the same for me but there is a fair amount of similarity. There is no clear course. I look at a little girl so full of life and joy and exuberance and some neon sign next to her head flashes, “probably not going to make it, probably going to die, don’t get your hopes up.” I look at this test result and hope. I look at that test result and fear the worst. One doctor emphasizes, “kid’s are resilient, they surprise you all the time,” and another keeps a straight face and offers no hint of optimism. I feel flung to and fro, bashing up against this likelihood of death over and over as I swing back around. It is not just a day-to-day existence here but a reality that from morning rise to evening’s setting sun the whole nature of things can change.
No matter how normal this has all become, no matter how cheerily I decorate her room, I constantly meet with shock the dark presence in the room. But I’m looking for joy, joy in the day and joy to come. I am fixing my eyes on the God who counts the number of hairs on my head and who determines each day, hour, minute, molecule, ion. It is His to choose where these days lead. It is His tale to tell. And what is my life anyway? Is it so very essential that I check the boxes I’m told relentlessly make up a good life? My life doesn’t fit into those wee constrained boxes and neither does my God. His ways are not our ways and there is thrill, there is invigoration, there is anticipation, there is leaning into these days. I am on the look out for what He will do. I am on the look out for my God who gave me this small, loving, beautiful, hilarious, strong, feisty, wondrous girl. Thank you Father for the abundance you have given. Thank you for better days and for a glimmer of light.






















































































































































































{kind=link}