40
40
1975
2013
2,650,000
6,800,000
8,000,000
So something cool happened. Forty years ago, in the year 1975, I was born. I know, sweet, huh? Just joking. I mean I’m pretty stoked I was born but what my parents could not have imagined as they gazed down at their newborn baby girl’s little face was that something else significant had just been created. Little did they know that blue-eyed baby girl cradled in their arms would one day desperately need what also had its beginning in 1975. In many respects I think it is grace that we do not know the future, that we don’t have to carry burdens in the present of situations yet to come. At that moment of my birth there was only joy, well my mom would probably say a little pain too. And yet isn’t it amazing that long before we have a specific need, the provision is often already on its way to being available and ready for us? And so it was that in 1975, Fred Hutchinson Cancer Research Center came to be and would one day dramatically intersect the life of that little baby girl and her baby girl. Beautiful. Makes me smile BIG!
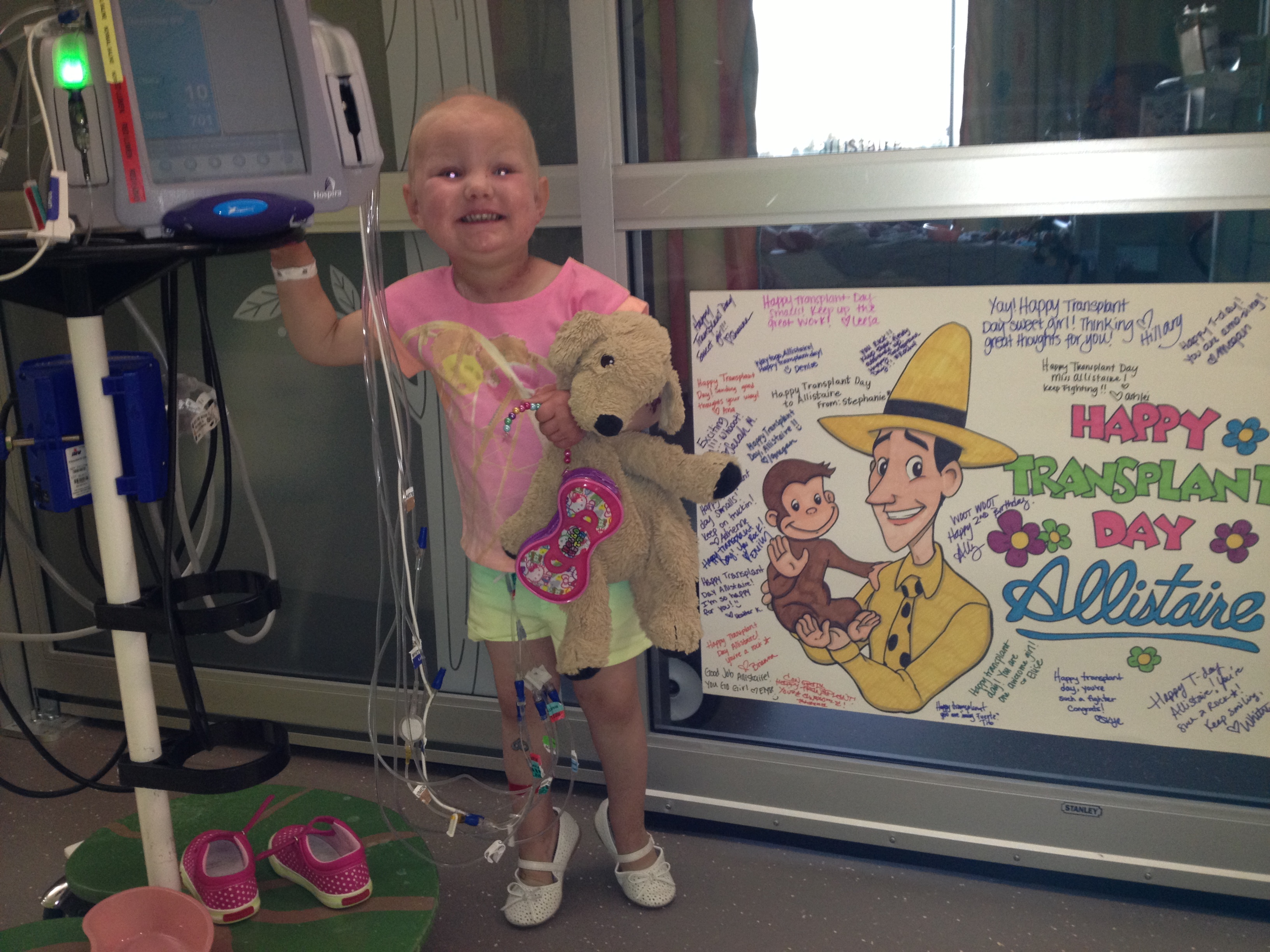
In the spring of 2013, there was a blue-eyed feisty three-year old girl named Allistaire. Turns out she had an aggressive type of leukemia that just wouldn’t back down in the face of every type of chemo thrown at it. It had come back after lying dormant after standard treatment and this time it was winning, filling her marrow and infiltrating the rest of her body with numerous tumors. The doors just kept slamming closed. But then, but then…a door opened. Allistaire had the amazing opportunity to have her disease filled marrow obliterated and then rescued with an infusion of donor bone marrow stem cells from a woman in Germany. This was only possible because of a wondrous clinical trial through Fred Hutch. Had it not been for that trial, for that single open door, there is no doubt Allistaire would be dead in the ground right now.
Time after time Allistaire has been the blessed recipient of the expertise and amazing research through Fred Hutchinson Cancer Research Center. I will always be indebted to that institution and its many phenomenal doctors and support staff! It is my joy to commend them to you and to keep seeking to add to their ability to propel research forward and provide more open doors for children and adults alike who find themselves facing that wretched beast Cancer.
And WOW! WOW! Look at what we’ve been able to do!!!!! This year, in August 2015, thanks to your incredible generosity, compassion and support, our Obliteride Team Baldy Tops raised $38,000! In total over the past three years riding in Obliteride, our team has raised nearly $60,000 for cancer research at Fred Hutch. This year’s ride raised $2,650,000, totaling $6,800,000 since the inaugural ride in 2013. One hundred percent of that $6,800,000 goes directly to cancer research at Fred Hutch! It makes me giddy. Sometimes one’s efforts feel small. It’s hard to put yourself out there and ask people to give of resources they could spend on themselves, and instead give it away for the betterment of others. Then again, you never know when you might find yourself in the desperate position of needing another open door in your own battle against cancer. When we put our efforts together they can have a BIG impact!!
Would you like to join us? Our team this year was super fun and included Sarah from Utah – an amazing woman I had never actually met until the morning of Obliteride. You should have seen her face when she finished her 50 miles – a beaming exuberant smile! Also on our team were two fantastic nurses, Lysen and Adrienne, from the Cancer Unit at Seattle Children’s where Allistaire receives treatment. Adrienne and her awesome dad rode on an old tandem bike (and I do mean old). Carrie, our amazing financial counselor at the hospital joined us as well along with her friend Eric, a local business man who wants to give back. And of course I had my dear sweet sister-in-law Jo by my side along with my oldest friend, Emily. Jo’s sister, Annie, also joined us. Her little baby boy, Marzio and husband, Franky cheered us on. It is such an amazing experience to be in a swarm of people gathered together for one purpose, each brought to that day by their unique stories. Obliteride has put together a short little video of this year’s ride to give you a taste of the experience. You’ll get to see several shots of our team (I have on a blue helmet you see a few times.) Click HERE.
The beauty is you don’t have to be a cyclist to participate in Obliteride. There are rides from 10 miles to 150 miles, from quick and easy, to covering two days and lots of hard-core hills. Wherever you are on the cycling spectrum, there’s a place for you to have fun and give directly to cancer research. Even your kids can get involved with the special kid’s ride. The 2016 ride is over the weekend of August 12-14th, so mark your calendars to ride with us or be a volunteer. Registration will open early 2016 and of course I’ll keep you updated! If you’re interested in being on our team Baldy Tops, please simply leave a comment on this post and I’ll include you in my Obliteride emails. Wouldn’t it be awesome for our team to reach the $100,000 mark with the 2016 ride?! I can’t wait! Here’s another fun video to give your more info on how to get involved in Obliteride.
This year is drawing to a close and you may be considering where to give your remaining 2015 donations. While it isn’t yet time to fundraise again for Obliteride, you can still give to amazing cancer research at Fred Hutch. One specific way is to support Dr. Marie Bleakley’s work. She has been one of Allistaire’s primary bone marrow transplant (BMT) doctors at Fred Hutch for the past several years. She is the BMT doc who is directing Allistaire’s upcoming (hoped for) transplant. Like most of Allistaire’s doctors, not only does she do an incredible job clinically caring for patients, but she does amazing research. One focus of her research is TCRs (T-cell Receptor T-cells). You will remember that this is the sort of immunotherapy Allistaire received with her WT1 T-cells. In the HA-1 T-cell immunotherapy that Dr. Bleakley is designing there are specific matching and mismatching requirements of the donor and patient which on one hand limit their applicability to a wide range of patients, on the other hand, they are not limited solely to patients with AML but could benefit patients with a variety of types of ALL (Acute Lymphoid Leukemia) and Lymphoma as well, thus expanding their impact. Dr. Bleakley says that, “There are actually numerous targets like HA-1 and different targets will work for different patient-donor pairs. We are trying to build a toolbox of TCRs so that we can ‘type’ the patient and donor and figure out which TCR will work for them.” This is personalized, targeted, sophisticated beautiful cancer treatment.
Dr. Bleakley has already been awarded a Bio Therapeutic Impact Grant of $682,000 from Alex’s Lemonade Stand (ALS) whose vast majority of funding goes directly to pediatric cancer research. I am told that 85 cents of every dollar donated goes to program and research grants with the vast majority of that going to the research end. Their program grants go to family’s to provide one lifetime grant of about $1,400 which we ourselves received two years ago in the form of plane tickets home for Allistaire and I. Dr. Bleakley is able through Alex’s Lemonade Stand to raise up to an additional $25,000 in donations through the end of 2015. For every dollar up to $25,000, ALS will match one to one. So in total she could raise $50,000 additional to go toward her research.
This is an incredible opportunity to fast-track her research in the lab to actual patients. The next step for her research is to take what they have been doing in the lab and bring it to a GMP (Good Manufacturing Process) lab. This independent lab would, with the aid of her research assistants, recreate their work in order to determine the safety and quality of the product they say they are producing. She said it’s like a dress rehearsal for the real process in which they would prepare the cell product for the patient. The information is taken and included in an IND (Investigational New Drug) Application for the FDA to approve. Once approved, they can then move forward to offering an actual clinical trial to patients. Basically they are at the point of taking their research in the laboratory and offering it as treatment to patients – that means an open door for patients with leukemia and lymphoma! An open door! You could help open that door. To learn more about her research click HERE. To donate and have your dollars matched one to one up to the goal of $25,000, click HERE.
You know what…At last count, Allistaire’s cancer treatment has cost just shy of 8 million dollars. That’s more money than all riders have raised in total over the three years of Obliteride. That is a crazy, mind-blowing number! My jaw drops every time I think of that number. Wouldn’t it be WAY COOLER if we could invest in research upfront that would reduce the cost of treatment, reduce the suffering, reduce the incredible investment of time of Allistaire’s life and our family’s lives fighting this fight? When we put money upfront to accelerate research, we open more doors! What if we didn’t have to rely on chemotherapy that isn’t targeted and takes down hearts and lungs and kidneys and livers and ovaries with the cancer cells. What if there was a way to deliver radiation so that it only killed tumors and not brains. What if surgeons could “see” exactly where tumor cells stopped and healthy cells started, getting all the cancer and sparing the rest? Wouldn’t it just be mind blowiningly awesome to use the incredibly complex, beautiful immune system you already have in your body to effectively and totally wipe out every last cancer cell so that “relapse,” is word never again uttered! When we put our money and effort into research, it isn’t just one patient that is benefited. Who can know how many people will be blessed by each step forward in cancer research. And this is a world-wide endeavor! Do you know that amazing minds are at work all over this earth trying to untangle the mysteries of cancer?! Israel, Germany, China, Italy…What is learned here carries value across the world and their efforts likewise bless us! Do you know that Fred Hutch has a cancer treatment clinic in Uganda?
As I have said many times, there are many worthy places to give of your time and money, many struggles on this earth that deserve and need our attention. It just so happens that cancer came barreling into my life and so it does for many, many of us. Cancer will touch us all, if not directly in our flesh, then most certainly in that of someone dear to us. One in three women will get cancer in their lifetimes as will one in two men. Thank you for the great swelling of your compassionate hearts that listened and responded in generosity and love. May you find many open doors!!!
As for our little bright love, Allistaire Kieron Anderson, well, she thrives, she runs, she hops, she laughs silly little giddy laughs and she told me today that the numbness in her face is finally gone. She looks incredibly good. Only every now and then can I detect that her right eye is slightly off. Yesterday she had a bone marrow test and today she had her PET/CT. We should know results soon. Hopefully the general trajectory going forward is one more round of chemo which will include Decitabine and Mylotarg again, though likely only one or two doses of Mylotarg this time instead of three. Then, God willing, she will have her transplant.
We’ve been at this point before. I am no fool to believe the road ahead is necessarily clear of barricades. It as though she walks through a field replete with land mines. To get across to the other side will take a miracle, so fraught with danger is the road ahead. Even yesterday, she had an echocardiogram which reported out an Ejection Fraction of 34 versus 45 last time. I don’t know how the BMT doctors will interpret this. The cardiologists say her heart function looks the same as it has on the last two echos despite variance in the numbers. Thankfully her cardiac MRI showed no scarring and affirmed great improvement in her heart. Going forward with chemo always opens the door to infections. Two and a half weeks ago she went inpatient due to an infection and the next day she had a separate issue with an extreme rise in her liver function numbers we finally concluded was due to her anti-fungal, posaconazole. Her ALT and AST were 1,156 and 1,450 respectively, the normal high being 40. It has been imperative to get these numbers down and get her liver happy again as Mylotarg’s one direct toxicity can be to the liver both in the setting of when it’s given and in transplant. Just getting to transplant is an incredible undertaking, then there’s the transplant process itself which holds many extreme dangers. If you get past all of that, you still have to contend with the possibility of GVHD and relapse. Thank you Lord that you have used these past four years to help me learn more and more how to walk day by day.
To learn more about the fascinating history and endeavors of Fred Hutchinson Cancer Research Center, click HERE