


 Batten Down the Hatches: Nautical Term – To secure a ship’s hatch-tarpaulins, especially when rough weather is expected
Batten Down the Hatches: Nautical Term – To secure a ship’s hatch-tarpaulins, especially when rough weather is expected
From hence forth, Allistaire is in lock-down mode. I will not allow her to go anywhere other than the hospital and our room at Ron Don. When she’s in the hospital she’ll be wearing a mask. The countdown has begun.
Last Friday I received THE call. The transplant coordinator called me with dates, actual “written on the books” dates for Allistaire’s transplant. Earlier that morning, Dr. Bleakley relayed to me that the pulmonologist at SCCA who cares for adult patients had reviewed all of Allistaire’s lung CTs and the testing results from her biopsy. He concluded that she does indeed have Cryptogenic Organizing Pneumonia (COP). Dr. Madtes felt confident that the testing had conclusively ruled out the possibility of leukemia, fungus and bacteria. He said that while it is not common to ever have COP and especially rare to have it more than a year post-transplant, he has seen it this far out. Also, the location of the nodules in her lungs he said are classic for COP. The treatment for COP is steroids which Allistaire began last Wednesday, December 2nd. He expects the steroids to be successful in clearing the infection and does not think it should require any delay going into transplant.
Thus we are able to move forward with her transplant. Next Wednesday, December 16th, she will be officially transferred into the care of Seattle Cancer Care Alliance and will begin a slew of testing that will take place over the course of the following two weeks. We do not have all the details of her schedule, yet the various tests will include a lot of blood tests, lung CT, PET/CT of her whole body, brain MRI, likely another echocardiogram and EKG, bone marrow aspirate and biopsy, and of course physical exams. The majority of these tests would be conducted anyway given that she is coming to the end of this round of chemo at the end of the month, but everything will be especially scrutinized in light of her ability to endure a transplant and the state of her disease which impacts the success of the transplant. All the testing will be wrapped up and conveyed to us in a “Data Review Conference,” on Thursday, December 31st.
While she is cleared to begin this process, this is really a process of final determination if she can have a transplant, it is not at all a guarantee of transplant. We all think she’s in a good place to move forward, but all this testing will verify that. This will be a very busy time full of appointments and sedations. Honestly, there are still a hundred thousand things that could stop us in our tracks. Last week Allistaire’s creatine level jumped to .9 which indicates the high possibility of kidney damage if you can’t turn it around. Because of the limitations of her heart, she was admitted to run fluids at a lower rate to help flush out the rising phosphorus, potassium and uric acid that were building up and putting stress on her kidneys. A day in the hospital helped her labs return to normal but this is just one example of how serious issues can arise out of the blue. The most immediate concern is her heart as her BNP (measurement of heart distress) was quite high last week at 824 (normal is 0-90). This lab was drawn the same morning that she had an echocardiogram that showed stable cardiac function and an ejection fraction of 43 and a shortening fraction of 21. The heart failure team think the high BNP was most likely due to getting fluids the day before, but this was a red flag for the BMT (Bone Marrow Transplant) team. Unfortunately today, it was still just as high at 830. I don’t know what’s going on but it sure is concerning. If it were to continue to trend up, again we could be stopped from moving forward.
Really and truly, there is no guarantee of transplant until the day conditioning starts. For those unfamiliar with bone marrow transplant, in general the process begins with annihilating the marrow and trying to eradicate the body of cancer cells. This first part of the process is known as “conditioning.” Sounds nice huh? It’s anything but nice. I’ll give more details another time, but suffice it to say, there is almost nothing more brutal you can do to a body than this full intensity “conditioning.” Conditioning is scheduled to begin on January 4th, with four days of “boost radiation,” to Allistaire’s sinuses where these awful chloromas/tumors have been in her face. She will then get the weekend off and have TBI (Total Body Irradiation) twice a day January 11-14th. Then comes the chemo, Fludarabine, January 15 – 17th. On the 18th she will have a “day of rest,” and the 19th will be the actual day of transplant when she receives the infusion of donor cells.
The transplant coordinator continued on with giving me dates, dates of approximately how long she’d be in the hospital and how long she’d have to stay in Seattle before she goes home. I mentally clamped my hands over my ears at this point. It’s just too much to consider. I can’t even look at the possibility of going home. I can only focus on the hope of getting her to transplant. After so many, many disappointments and cancelled plans and hopes, I rarely look more than a few weeks into the future. The cardiology scheduler called the other day to set up appointments for January and February and I laughed out loud, a sad, cynical laugh – I cannot even anticipate what this Friday holds, much less a month of two from now. Allistaire has been talking more and more lately about how excited she is about transplant because it means she can go home after that. I am totally honest with her and tell her we don’t even know if she’ll be able to get her transplant, whether or not she’ll survive the transplant and even more so whether or not it will work.
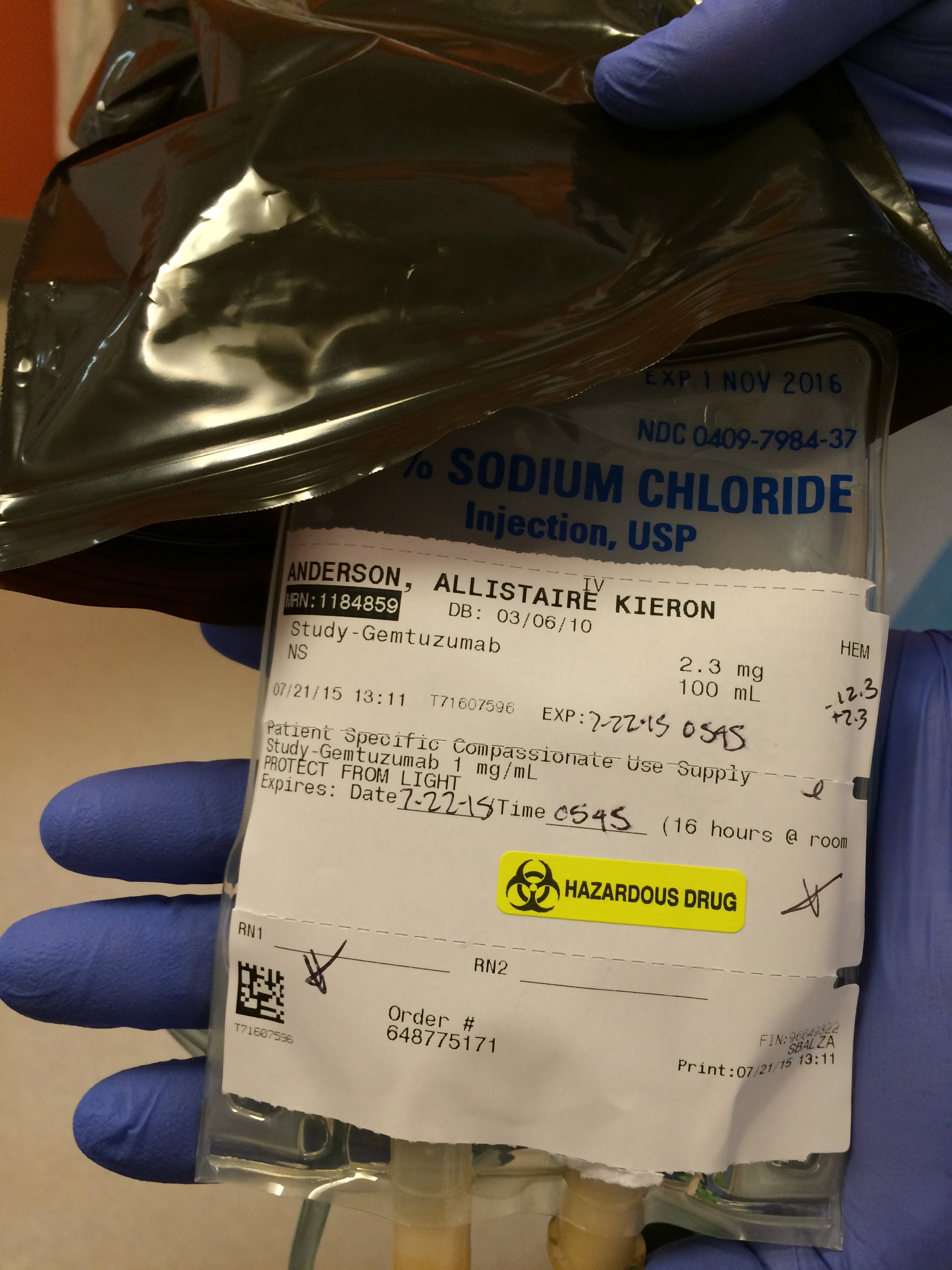
The truth is I feel beat down these days. These holidays are driving me sort of crazy. I love the delight they bring Allistaire as we decorated her little pink Christmas tree with lights and ornaments and listening to Christmas music. But everywhere I turn the holidays are just screaming in my face how far from normal our lives are, how far from the life I long for. Today has been a hard day. Yesterday evening I talked with my friend whose daughter is here for her one year post-transplant follow-up and her bone marrow test confirmed relapse as they feared. They are scrambling for options. I also found out last night that our sweet little AML friend, Ron Don neighbor and fellow Montanan has blasts in her blood and numerous chloromas. Stevie is only four and has the cutest voice you can imagine. This is confirmation that this round of chemo did not work. Like Allistaire, she is trying to get to a second transplant. I keep imagining how hard this week is for Heather as she and John prepare for Lilly’s memorial service on Saturday. Allistaire’s high BNP just makes no sense to me and terrifies me that issues with her heart could show up and this whole transplant attempt could come crashing down. She cannot just keep getting Mylotarg. This feels like her one last shot. Everywhere I turn, disaster, desperation, deepest wells of sorrow.
I was listening to a song today that had as its core the verse John 15:13 which says that, “Greater love has no one than this: to lay down one’s life for one’s friends.” Then Romans 8:16-17 came to mind where it says, “The Spirit himself testifies with our spirit that we are God’s children. Now if we are children, then we are heirs—heirs of God and co-heirs with Christ, if indeed we share in his sufferings in order that we may also share in his glory.” Why did Christ suffer? Why did God ever take on the form of a frail, temporal human in the first place? Was it not all because He loves us? Because His heart is moved by compassion and He longs to be in relationship with us? He came in the form of man as Jesus Christ in order that through His suffering, His death, we have a way into eternal life with Him. His whole life and His death were for the express purpose of being light to the world, to display and demonstrate in action the love and holiness of God, all so that we would see, that our hearts would turn to Him and receive life!
Christ suffered while He was alive and He suffered ultimately on the cross. He demonstrated ultimate love by laying down His life for those He longed to call friends. I am not being persecuted for my faith in Christ and yet everywhere I turn, I cry out, “Lord God! It is all a mess! It is all ragged and torn and in disarray. This is NOT THE LIFE I WANTED!!!” I want to rage at Him. And then I bend my knee, my face to the ground. “You are God and I am not. Your ways are higher than my ways. You are other!” Who am I to say what my life should look like? Is not all my life, all my life to be a reflection of the wildly compassionate heart of God? Who am I to say how He is best displayed? Nothing in my life resembles the sort of life I thought I would have, the life I envisioned for myself. There is nothing here to display on Pinterest. When I survey my life, it hits none of the bullet points I wanted.
But then, then I must get down low, I must crane my neck up scanning the night sky and ask, what really, really do I want out of this life. Hasn’t it always been about the two commands, to love the Lord my God with all my heart, soul and spirit – with all my strength. And to love my neighbor as myself. If this is what I claim my life is about then guess what? This is exactly a perfect place for my life to be. Every single day, from the moment I wake up until I finally fall asleep is a constant seeking after the Lord, constant calling out to Him, constant praising Him, constant wrestling with Him. This is what a broken life for a child of God accomplishes: an abiding, I in Him and He in me. And He has allowed me to walk into terrifying dark and made Himself known to me there, here, that I in turn might share His comfort with others in this black place. Because it is so black, so utterly dark, it challenges one’s very core and all that is connected. I am able to love those in the dark in a way I never could have before entering the darkness myself. Sometimes the pain of this place is blinding and consumes the view. Sometimes the pain seems to ring through every last nerve, the tips of your fingers searing with hot sorrow. I seek to mourn with those who mourn and rejoice with those who rejoice.
Sometimes I scream, scream, scream in the car. Scream so hard my throat is raw. There are no words for the depth of this tearing. Father, you have brought me into this land I never sought, a land I have despised, a land that made me cringe and hoped I would never have to know anything about. It is a barren land, ugly and dangerous. And yet, in this land I have seen your face, heard your voice; I have begun to taste of what it is to walk with you. In this land I have been able to offer my hand to those who also travel this bleak road. The treasures of my life will get me no where with a retirement plan, they will not draw people to me because of my accomplishments, my travels, my career, my beautiful house, my knowledge of politics, world events…My bounty is only in the Lord and to the eyes of this world it looks empty, flimsy, small. But what if this mess of a life enables me to enter into places to love? What if this is the way I share in the suffering of Christ who laid down His life for His friends? How can I say no to that?
As I sit here, ever trapped in Ron Don, a few short weeks before we will know if Allistaire’s life opens forward toward transplant or gets shut down to a remaining few more months, I reflect on the past four years. Yesterday marked four years exactly from the day Sten and I sat down in a hospital room with Dr. Gardner and Dr. Tarlock to be told that Allistaire had Acute Myeloid Leukemia. In the midst of incredible sorrow, of feeling utterly overwhelmed, the Lord spoke to me in the quiet – “Be expectant, be on the look out for what I will do.” Had I known that day what the coming years ahead would hold, I could never have imagined how I would endure. But He told me that He promises bounty. I have never taken that to mean a guarantee of Allistaire’s life. I fix my eyes on Christ – on God who is other, who is eternal. He may grant us Allistaire’s life and He may not but I put my hope in the fulfillment of His promises to redeem and make new.
The intensity mounts, the ringing tension builds up and up and up. I long for resolution. I long for a day that I get to tell Allistaire we can go home, not to die, but to live. How glorious such a thing would be! But today we must dwell in this day, this gray flat Friday afternoon with trees bare. Father see us, have compassion and help us to endure, and not just endure, but to know your bounty, bounty here and now and hope for eternal bounty.
*I now have word that Allistaire is scheduled for her brain MRI next Tuesday, 12/15, and her bone marrow aspirate and biopsy next Friday, 12/18.































































































































































{kind=link}
{kind=link}
{kind=link}