



 I grew up in a land of unfoldings. A land where one must bend low, look now, another unfurling. A land of delicate magic, intricate. Stepping over branches slick, footsteps quiet on the soft underfloor of forest. Ferns unwinding, their beings all folded up tight in complex arrangement, arching their backs, rising toward the light filtering down to them from high in the silhouettes of tree tops. Little ferns with leaves paper-thin, bright green in direct light, countless shapes repeating. Fuzzy juicy stalks and delicate sleek black ones. Mosses creeping, covering like downy shawl a glorious, vigorous green. Everywhere lush. I recall making a fern fort once. Ripping up scores of Lady Ferns, weaving them into walls and overhanging. I lay down upon the mossy floor and looked up through that scattered light, the greens bright like stained glass. Ferns and moss, resplendent greens of life unrelenting, delicate yet most resilient. Two gifts of this earth instantly inciting glee in my heart. Like Thoreau, I repeat, “I think my own soul must be a bright invisible green.”
I grew up in a land of unfoldings. A land where one must bend low, look now, another unfurling. A land of delicate magic, intricate. Stepping over branches slick, footsteps quiet on the soft underfloor of forest. Ferns unwinding, their beings all folded up tight in complex arrangement, arching their backs, rising toward the light filtering down to them from high in the silhouettes of tree tops. Little ferns with leaves paper-thin, bright green in direct light, countless shapes repeating. Fuzzy juicy stalks and delicate sleek black ones. Mosses creeping, covering like downy shawl a glorious, vigorous green. Everywhere lush. I recall making a fern fort once. Ripping up scores of Lady Ferns, weaving them into walls and overhanging. I lay down upon the mossy floor and looked up through that scattered light, the greens bright like stained glass. Ferns and moss, resplendent greens of life unrelenting, delicate yet most resilient. Two gifts of this earth instantly inciting glee in my heart. Like Thoreau, I repeat, “I think my own soul must be a bright invisible green.”
And birds. Oh the birds. Fat breasted robins calling in the early morning when light has only begun to seep. Chatterings, bushes alive with tiny throbbing birds. Evening calls as day calms toward night. The days are lengthening. Crocuses and daffodils thrust up from the dirt. Cherry blossoms pink, forsythia and azalea. Tiny white clusters like thick stars on the limbs of apple trees. This is something Washington has that our home in Montana never will. Spring. Winter turns almost suddenly to summer in Montana and doesn’t come until June. But here, in this land, the drear of February, a time when the weariness of winter starts to become intolerable, it catches you off guard…there, did you see it? Stirrings. Hints that winter will not forever stake its claim. In the cold of ground and the rigidness of trees and branches, life still courses. Somehow what looked vacant, dead, unmovable, is everything to the contrary. Nay, there is an overcoming, some inner working unseen to my eyes, yet with such vigor as to burst through rock and soil and press out of wood and limb. A draw from distant lands, a call for the birds to return.
Spring is as sure as anything in this life. We know it deep in our flesh, our own veins course with anticipation. An inclining. An unconscious arching toward light, a yearning to feel warmth of light and freshness of breeze. Some mineral tang on the tongue that declares life never ceases, though all appears to disagree. That’s what we’re banking on, that is what moves us through our days. A hope. Hope. Such an overused word. But no, no. It is not merely some ancient knowledge that the earth will continue spinning on its axis, marking countless days and nights and a relentless orbit that will always swing back toward sun. No. Hope is unique to our humanity. Hope looks about and not only says, but proclaims, what I see now is not all that there is, there may indeed be more and different. Hope looks forward. Hope is the very essence of endurance.
There are stirrings in the woods, stirrings of song and light and delicate unfurlings that press against the dark and the cold. It makes me giddy. Giddy that death will never ultimately overcome. Giddy that the world is arcing in its orbit toward the sun. Giddy that one day the land will be bursting with life and the sun will rule the day and their will be an unstoppable flourishing. Abundance will mark life. No longer scarcity. No longer mere grasps at survival. No longer decay and death. The greens are unfurling. The birds have begun to call out to the morning. Spring is that tangible bright expression of the hope that courses through me.
And I have much to be giddy about. Hope abounds.
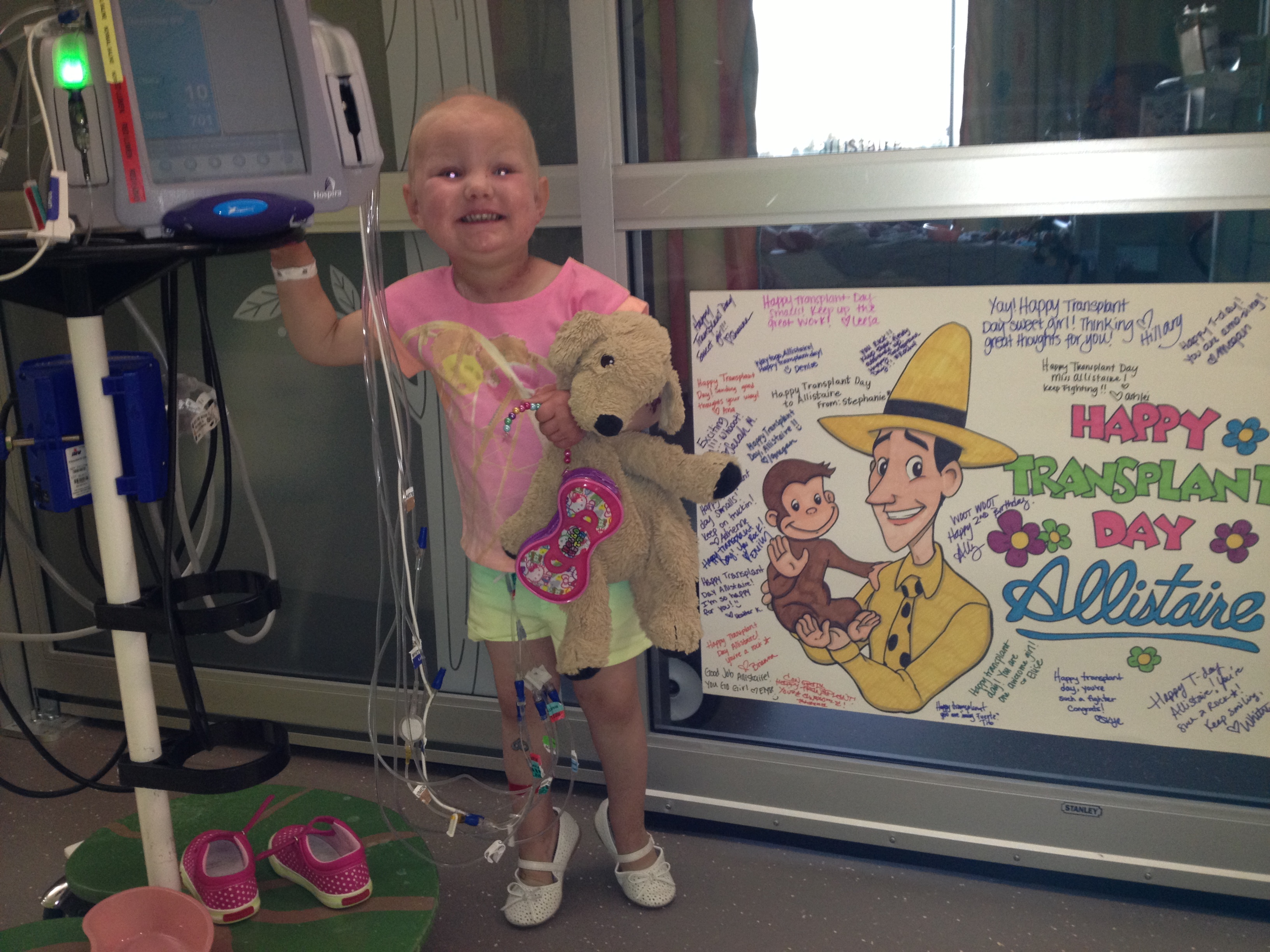
The land is wakening and it lightens the step and everywhere there is more to smile about. And Allistaire is doing just so surprisingly well. Dr. Sohel Meshinchi, our current BMT (Bone Marrow Transplant) clinic attending doctor, has ended our last several clinic visits with the statement, “I have no concerns.” This is like balm to the feverish forehead of a cancer parent. Her labs continue to look great and even improve. Her red blood and platelets are recovering, with platelet transfusions being spread out to one or two a week, whereas they had been every day to every-other day. Robin, our clinic nurse the other day said with glee, “Look Jai, look here at her ANC (Absolute Neutrophil Count), it’s normal.” She looked at me with shining eyes. Normal. 2,612 What an amazing number. What a wonder?! Normal. Imagine that!!!! Her liver function numbers have improved substantially and are only slightly high, her kidneys continue to do well and her BNP (measure of heart distress) was down to 119 the other day, a gorgeously low lab value. She continues to be CMV negative (Cytomegalovirus which can reactivate). Her weight is good as her appetite improves and taste buds return to normal. She has begun to eat salad, and even declares its tasty with the exception of the one half of one grape tomato I force upon her which causes her to dramatically grimace and gag every single time. She skips and paints and rides her bike and sings really loud with her headphones on.
Today marks Day+43 post transplant. We are still very early in this very long process. My brother asked me a while back, when we would know if the transplant was successful. Success is multi-pronged in this situation. The first mark of success is that she has survived the actual transplant process itself. Her body and specifically, her heart was not overwhelmed by the cytokine storm of the infusion of the donor cells, nor the hyper-hydration necessary with the chemo. The cyclophosphamide did not cause the slim but terrifyingly possible acute heart damage. Her lungs did not bleed nor did she have the brain damage possible with MMF. Her liver remained healthy despite the increased risk of VOD brought on by several rounds of Mylotarg. Her graft did not fail, rather Sten’s cells have latched on forcefully resulting in 100% chimerisms. Her marrow is clear of detectable cancer both by Flow Cytometry and cytogenetics. Thus far, her transplant has been a success. It is a beautiful surprise. Allistaire’s golden birthday is coming up soon and honestly, as I look back, this is the fifth birthday that I never knew would come and had much reason to think it never would. It is the fifth time we have had cause to celebrate life that might not have been, life that has been relentlessly hounded by cancer. But hope has continued to mark our days, and now years.
This next phase of transplant continues to be about making sure the cancer is kept away and about being on guard for GVHD (Graft Versus Host Disease). Every two weeks she gets a LP (Lumbar Puncture) in which Intrathecal Chemo is given and a sample is withdrawn to check for disease. This means chemo is placed directly into her spinal fluid as it can be a “sanctuary for leukemia,” given the blood/brain barrier that does not otherwise allow chemotherapy to pass through. While CNS (Central Nervous System) relapse is less common in AML (Acute Myeloid Leukemia) than in ALL (Acute Lymphoblastic Leukemia), the more common form of childhood leukemia, it is still a danger. She will get 5 LPs in all post-transplant. So far, her LPs have not detected any cancer in the spinal fluid. She will also be getting a BMA (Bone Marrow Aspirate), and PET/CT on March 15th. Typically BMAs are done post transplant only on Day+28 and Day+80. But for high risk patients they include another intermediate BMA. March 15th will be her first PET/CT since November and before her last round of chemo pre-transplant. At that time, her body was clear of chloromas with the exception of those in her sinuses, which had reduced in bulk from the previous round of chemo but were still present along with one new small chloroma. While her sinuses received 5 fractions of focal radiation and her body was barraged with TBI (Total Body Irradiation) and systemic chemo (fludarabine and cyclophosphamide), I am still nervous about this upcoming scan. Her cancer has defied countless assaults, its tenacity awe-inspiring and terror invoking.
At this point, there is no evidence of her disease. I rejoice at this and simultaneously remain on high alert, knowing “no evidence of disease,” in no way means we can confidently say there is no disease. The other significant issue the doctors and I are ever watchful of is GVHD (Graft Versus Host Disease). GVHD is when the donor cells attack the host (Allistaire), most commonly in the skin, gut and liver. GVHD is always a concern in bone marrow transplants but especially so in Allistaire’s case because of the much greater mismatch to Sten. Common symptoms of GVHD include skin rashes, tummy pain which can cause the patient to stop eating, diarrhea, and elevated LFTs (Liver Function Tests). There is a strange love-hate dance with GVHD. GVHD can severely impact quality of life and even cause death. What starts out small can suddenly turn into “rip-roaring GVHD,” so caution and response is necessary. But the treatment for GVHD has its own consequences. Immune suppressants such as prednisone and cyclosporine are given to tamp down the aggravated response of the T-cells. However, not only can these drugs have devastating effects on bones and joints (it’s not uncommon for teenagers to get hip and knee replacements), but the rest of the patient’s immune system is suppressed along with the T-cells causing the GVHD. This means the body’s ability to fight infection is radically diminished, again sometimes resulting in death from infection. In addition to the complications to be avoided from responding with medication to GVHD, the doctors actually want some GVHD. The thing is, when the donor cells are ramped up and attacking the host/patient, there is also the potential for the GVL effect (Graft Versus Leukemia) or GVT (Graft Versus Tumor in non-leukemic transplant patients). This is the secret weapon of stem cell transplants, an army roving the body to wipe out anything foreign which includes any lingering cancer cells. The hope of a transplant as a cure for cancer does not rely solely on the intensity of the conditioning, but rather, the more sophisticated element of the transplant is its micro soldiers that infiltrate the whole body and have the lasting ability to eradicate cancer. This is the “immunotherapy” element of a transplant. This is where I swoon. Don’t you just love it? And it has taken decades of research to begin to tap these mysteries.
A virus has taken up residence in Allistaire. Interestingly, it is a virus which even the most sensitive viral tests at SCCA cannot identify, never the less, she has had copious amounts of snot and some coughing. It is her first cold in over a year at least. With this virus we have seen what may be a small flare of GVHD, evidenced by a red spotted rash on her cheeks, spreading out from near her nose. Additionally, there seems to be a bit of a bumpy, slightly patchy pink rash on parts of her arms, back and chest. I was instructed to watch carefully for its advance both in terms of spread and speed. When Allistaire received the infusion of Sten’s stem cells (say that 5 times fast), she was given some mature blood cells from his peripheral blood but primarily his stem cells. Because the mature blood cells she received from her have mostly died out at this point, the immune fighting cells in Allistaire’s body are immature and have never been exposed to pathogens and are presently “uncoordinated” in their assault on this viral invader. Hence, both the virus and places like her skin are under attack. Apparently this pairing of having a virus and a flare of GVHD is very common. In fact, when there is evidence of GVHD, the doctors then go looking for an infection.
The other possible cause of this potential GVHD flare is the removal of one of her immunsuppressants and the tapering of the other. According to the protocol for her transplant, her MMF was to be stopped at Day+35. Typically at SCCA they would rather taper the MMF rather than stop it abruptly. However, Allistaire has clearly and repeatedly demonstrated that she has very aggressive disease putting her at extremely high risk for relapse even now. Removing the immune suppressants releases the hold on the T-cells which we hope will identify and wipe out any remaining cancer cells. For this reason, the doctors are very motivated to remove all immune suppression as rapidly as is safe to do so. So about a week ago her MMF was stopped all together. Then this Monday, 2/22, we began to taper her tacrolimus on Day+41, whereas the protocol calls for the taper to begin on Day+180. During this tapering process, she will be “watched like a hawk,” as the BMT staff seems to like to say, looking for any signs of GVHD and potentially backing off or slowing down on her taper if necessary. I am told that in these Haplo transplants, it is more common to see GVHD later than in unrelated-matched donor transplants (probably because of the post-transplant cyclophosphamide). More typically, acute GVHD is seen around Day+60 and later.
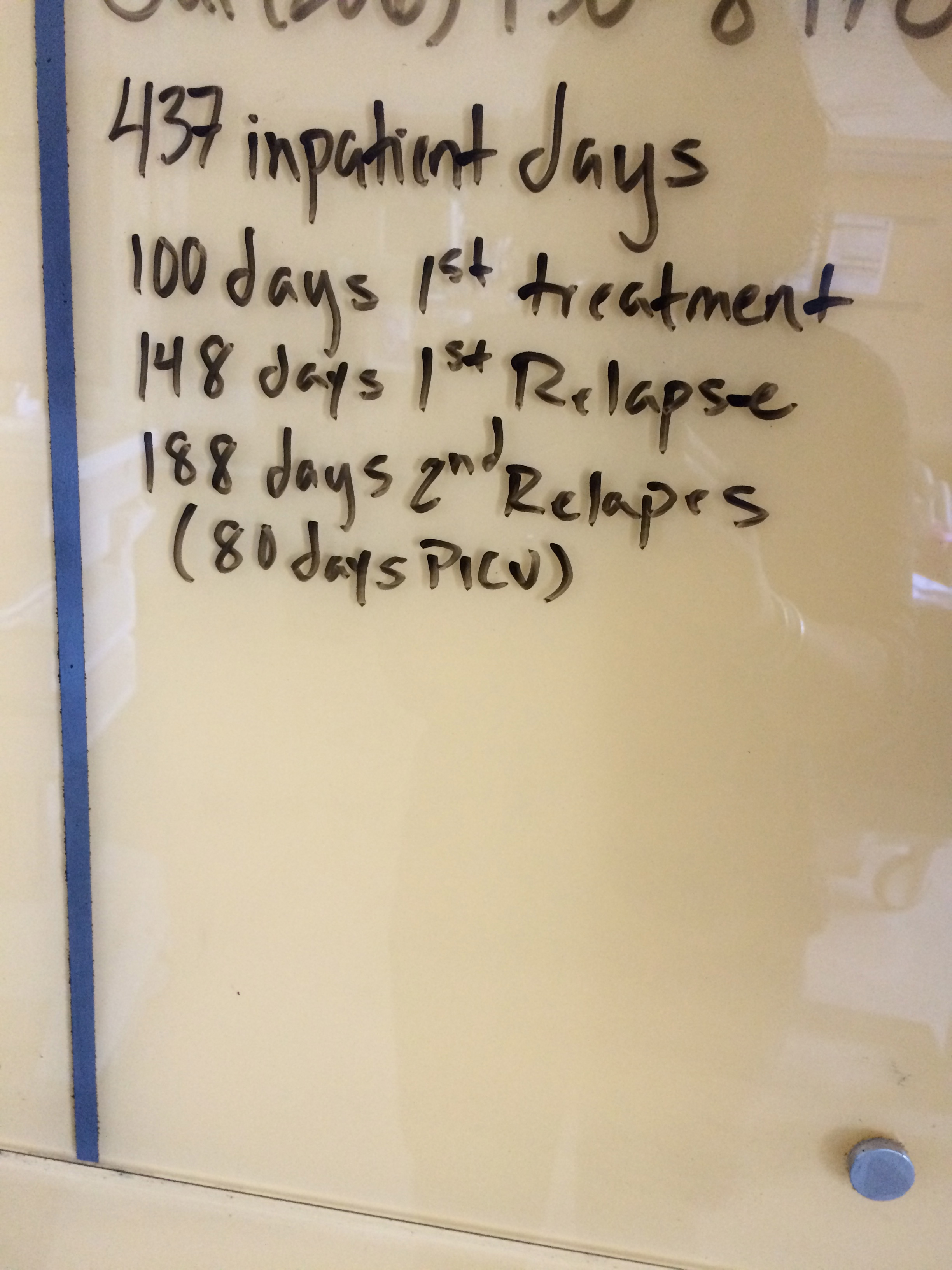
There is in the transplant world a magic number. One-hundred. One-hundred days is a song, like some mantra, some enchantment, a mystical goal out there in the fog. The standard is that, baring any serious complications, a patient’s Hickman line is pulled on Day+100 and is allowed at long last, to return home. I haven’t calculated the date exactly, but I know in Allistaire’s case, Day+100 is somewhere around mid-April. It’s out there. The date I avoid, I skirt around. I only allow it to linger in my periphery. I will not look it straight on. I am too well acquainted with disappointment. I keep my head down and we trudge on, willing ourselves not to be tired, not to be discouraged.
In August 2013, I was told in the most direct way, that Allistaire’s only chance for survival was a second bone marrow transplant. At that time, she was only Day+50 post her first transplant. You must wait an absolute minimum of six months between transplants to even have a chance of survival. For us that meant December. December was impossibly far off and the idea of going through it all over again was the most overwhelming moment of my life. People say the day of diagnosis is the worst. I most heartily disagree. When you are diagnosed, most of the time you have a plan, a means of response, hope that you can make it through. But what about when you’ve done the thing you came to do? You tried the big gun. And it just didn’t work. It wasn’t enough. And now your foe is even stronger than when you first began because it has mutated and become resistant at the very same moment that you are at your weakest, your most worn-down. But then Allistaire went back into remission with one round of chemo and there continued to be no more evidence of her disease as she completed a total of seven rounds of chemo post transplant. So when the day came for her one-year post-transplant follow-up and all looked well, I kept quiet. I was so very tired you see. I never asked about that second transplant. I just smiled and let myself finally feel a bit at ease.
Looking back, I understand the depth of that woman’s fatigue, but part of me screams, “You fool!” What if we had done that second transplant then? Her body was in great shape. No heart failure. No evidence of disease. A perfect time really for a second transplant. But I didn’t ask. I was tired. I just wanted to run as fast as could out of that cancer world and have a shot at normal life. Well, really I can’t remember if I asked or not. But even if I did, I must have accepted that answer. I’m not going to let that happen this time, no matter how weary I may be. I keep pressing the question. What are we doing to help prevent relapse? Okay, okay, we’ll do that, but what else can we do? What about this? What about that? As with so much in the world of cancer treatment, we are dealing in the world of utter unknowns. Dr. Meshinchi told me today that Allistaire’s specific MLL (Multi-Lineage Leukemia) translocation where chromosome 11 just broke off and attached to another chromosome, is unique among the 3,000 pediatric AML samples he has in his database. There is no data to say what someone is Allistaire’s very unique situation most benefits from. And every form of treatment has the potential for side-effects and the question is always, are those potential risks worth the unknown, untried benefit?
For now the plan is this: we will rapidly taper off all immune suppressants as fast as possible while trying to avoid GVHD in any severity. The hope is to allow the T-cells to have the brakes taken off of them and allow them free reign to roam wide and vigorously to eliminate any remaining cancer cells. Ironically, if there is no evidence of GVHD, we are planning on a bold move, rarely attempted, to elicit a GVHD response. The goal is to be off of all immune suppressants by Day+100 and if at that time there has been no evidence of GVHD, Allistaire will be given DLI (Donor Lymphocyte Infusion). DLI is an infusion of just lymphocytes from Sten. There are probably enough stored cells from his stem cell donation to get the necessary number of lymphocytes. If not, he can do a simple blood donation which would not require GCSF shots because it would not include stem cells. These donor lymphocytes would be infused into Allistaire in hopes that the white-blood cell hunters will recognize Allistaire as foreign and go on the war-path. Soheil does not recall them ever trying this “prophylactic” DLI approach. DLI has been given in the context of minimal residual disease in hopes to wipe out tiny bits of cancer, but never or very rarely when there is no actual evidence of disease. If she were to get DLI and it was well tolerated, she would be given a larger second dose about a month later. This also means that we have a good chance of having to be out in Seattle longer. It is all a matter of waiting and seeing.
A few weeks ago I found myself feeling extremely down, baffled and frustrated with my deep sense of sadness. We had just been discharged from the hospital and moved into our apartment at Ronald McDonald House. Allistaire was doing amazingly well, yet I could not shake saturating sadness. It was an act of will to hold back the tide of tears threatening to swamp my little boat. Perhaps like a runner in an ultra-marathon, having finally made it through transplant, I found all my reserves of energy come crashing down. I felt tired to my very core. When I tried to force myself to look up, all I could see were the sad, tired faces of my friends who have lost their children. I kept thinking of Stevie and Lilly reduced to ashes. How many? Sara, Ruby, Mario, Benton, Jaxon, Tristin, Christian, Pantpreet, Nolan, Jordan, Marleigh, Howie, Cyrus, Zach, Karlee, Bella, Lilly, Stevie. These are the children who have died in the time Allistaire has been in treatment – children and/or their parents that I have known – not even close to the total number that have died. These are the faces I have known. Though I have much to rejoice in with Allistaire’s progress, it has sometimes felt like her death is inevitable, just a matter of time. Sometimes my whole vision is consumed with the bright faces of children gone still. Home and a life freed from the grips of cancer sometimes seems like an impossible dream.
But there are stirrings see? Whisperings. Eyes a blaze with zeal. Minds whirling with ideas. Happenings. Little discoveries and victories that are starting to turn the tide. As the earth has reached the furthest reaches of its orbit, it has begun its journey back toward the sun, the earth warming and throbbing with life, unfurling. There are stirrings too in the world of cancer research. Great wonders have begun to be revealed. While it has literally taken decades and decades of research to get here, there is now starting to be a new world of promising cancer treatments which look in and down to the genetic level, down to the world of molecules. Immunotherapy, in which the intricacies of a patient’s own immune system is harnessed to track down and obliterate cancer while sparing healthy cells, is making incredible advances. Like a wild-fire that starts with a mere spark, so it seems is the world of immunotherapy. There is hope that the world of cancer treatment is on the verge of a tremendous revolution. There is hope that we are on the cusp of seeing a future for cancer patients that will look radically different from that dominated by the standard weaponry of chemotherapy and radiation.
Right at the center of this immunotherapy revolution in cancer treatment is our much beloved Fred Hutchinson Cancer Research Center. Check out this article from The Huffington Post that tells about the successes of Dr. Stanley Riddell of Fred Hutch which has yielded amazing results: putting cancer patients who have failed all other forms of treatment into remission at staggering rates using T-cells. Everywhere I turn at Fred Hutch there are new amazing trials and areas of research underway. Allistaire’s clinic attending, Dr. Soheil Meshinchi, and our dear Dr. Marie Bleakley are working on designing TCR T-cells that target highly specific proteins found only on leukemic cells. I sit and ask Soheil question after question and listen with mouth gaping, on the edge of my seat, eager to hear where the world is headed.
But there have also been moments as I’ve sat in wonder that I also find myself grieving. All of these advances are far too late for the eighteen children whose names I listed above. Much is even too late for Allistaire. Just four years have passed since she was first diagnosed and already the treatment of AML has changed. There are new tests done at the point of diagnosis to better determine what course of treatment works best with the individual’s unique disease. There are new treatment options that simply did not previously exist. It was only in April 2012 that the very first child was treated with genetically modified T-cells. I wonder what it would be like if Allistaire were diagnosed today, rather than four years ago. How much better would her chance of survival be? I also hear Soheil mention over and over again, “it’s a matter or resources…if we had the resources…” Resources!!!!! Sometimes I want to scream. So you mean, if you had the resources you could do this and this and this and give my child the treatment she so desperately needs? But you see, resources are scarce and government funding has been in short supply. These very brilliant, intelligent brains that should be devoting their time and energy to research, to what their good at, have been having to run around trying to scrape up money to keep their labs going, to find a way to pay to design that test, that piece of equipment, get the research from the lab to treatment in the clinic.
You know what I want to see? I want to see cancer research accelerated so that fewer kids and moms and brothers and friends have to have their lives cut short. I want to see treatments that actually cure! I want to see treatments that cure without poisoning hearts and kidneys and brains! I want to watch in wonder as scientists learn to use our very own beautiful, wild, amazing immune systems to obliterate cancer. And science is science – all these advances in understanding the genetic base for not only cancer, but for so many diseases, and how to make genetic modifications and therapies promises to benefit lives touching each one of us!
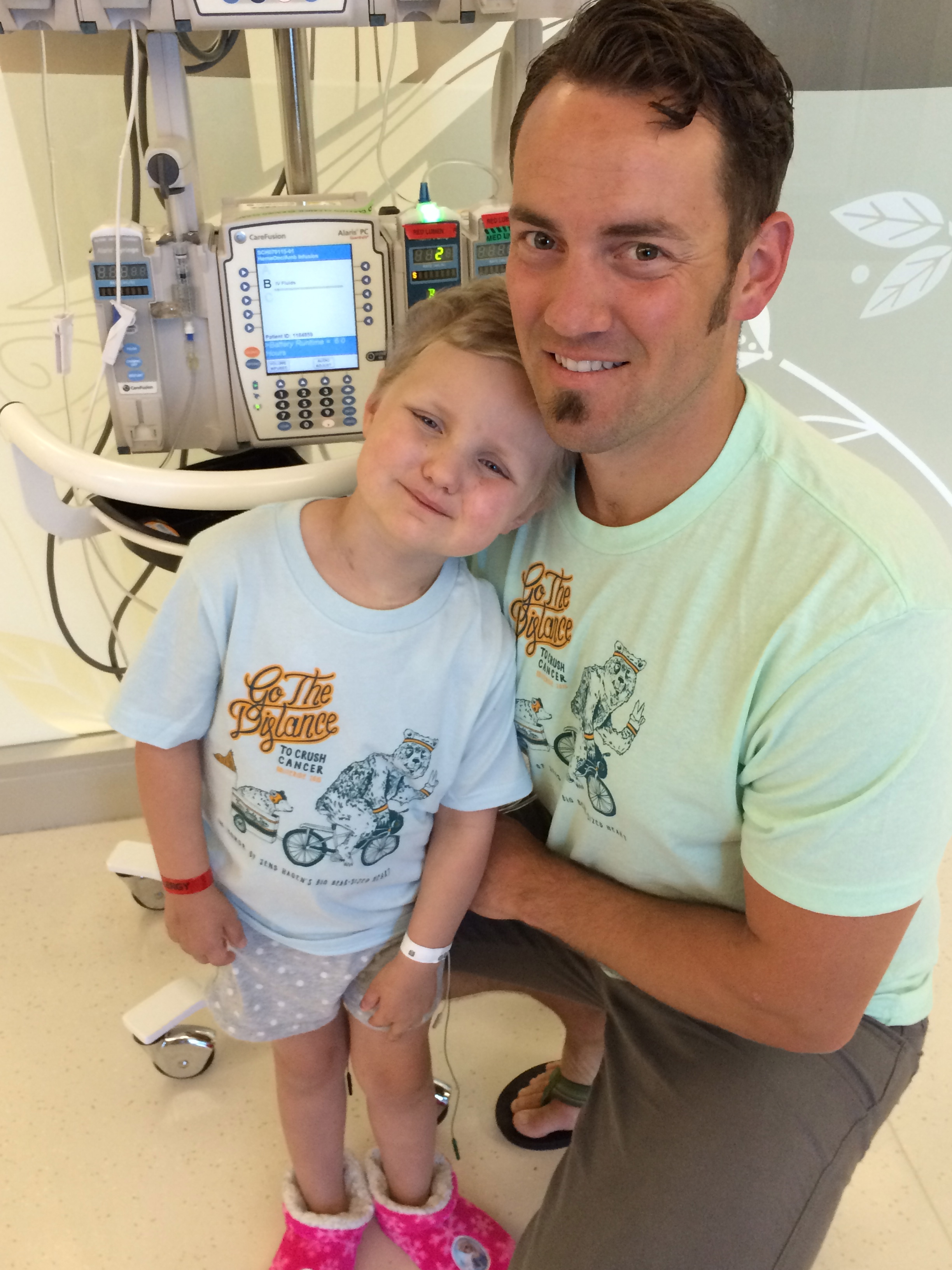
I’m going to get on my bike again this summer of 2016 and ride to accelerate research, to save lives faster, to obliterate cancer. I’m on Team Baldy Tops again this year in Obliteride and I’d love to have you join us! Come on out the weekend of August 13-14th and ride with us. There are routes for every skill level, from 10 miles to 150 miles. If you’re not up for riding, you can still join our team as a virtual rider and raise funds for cancer research. And easiest of all, you can donate! One-hundred percent of all funds raised in Obliteride go to cancer research at Fred Hutch!
Hope is being able to imagine a world that looks different than it does now. The cold and dark of winter is turning toward the bright zeal of spring. One day kids diagnosed with cancer won’t have to die, but can be cured and go on to flourish in this life. One day your mom, your wife, your sister, your daughter won’t have to fear breast and ovarian cancer and having to make the brutal choice of whether or not to cut out chunks of her womanhood. One day you won’t have to watch your dad whither away or lose your best friend. While my ultimate hope for life overcoming death rests in Jesus Christ and His promises of redemption, resurrection and a new heaven and a new earth, it is joy to see His grace in this lifetime as this vicious disease has begun to meet its match.
I will ride in Obliteride again this year because I will forever be indebted to Fred Hutchinson Cancer Research Center. Allistaire would not be alive today were it not for the research, the clinical trials and the treatment she has received through Fred Hutch. I ride in gratitude for my child’s life. I ride in sorrow for the children I’ve known who have died. I ride in hope for cures for cancer!
Check out this great video of Allistaire promoting Obliteride, now showing in movie theaters in the Seattle area.
Donate HERE to support me in Obliteride to end cancer!
Check out all the details at Obliteride.org
See what Obliteride looked like last summer and catch glimpses of our awesome Team Baldy Tops
Learn more about Immunotherapy





































































































































































































{kind=link}