
 (Top pic: Allistaire 14 days after the first of three doses of Mylotarg; Bottom Pic: The day before the first dose of Mylotarg)
(Top pic: Allistaire 14 days after the first of three doses of Mylotarg; Bottom Pic: The day before the first dose of Mylotarg)
In late August of this year, eleven native Christian missionaries near the town of Aleppo, Syria were killed for their refusal to deny Christ and return to Islam. Three were crucified and eight were beheaded after the women were publicly raped. According to villagers who witnessed this, one woman reportedly “looked up and seemed to be almost smiling as she said, ‘Jesus!”
Perhaps you don’t believe this report. I immediately thought of Stephen who stood up for what he believed, that Jesus Christ was the prophet God had promised to His people Israel and to Moses. In the face of his life being threatened, he refused to back down.
Acts 7:54-59: “When the members of the Sanhedrin heard this, they were furious and gnashed their teeth at him. But Stephen, full of the Holy Spirit, looked up to heaven and saw the glory of God, and Jesus standing at the right hand of God. “Look,” he said, “I see heaven open and the Son of Man standing at the right hand of God.” At this they covered their ears and, yelling at the top of their voices, they all rushed at him, dragged him out of the city and began to stone him. Meanwhile, the witnesses laid their coats at the feet of a young man named Saul. While they were stoning him, Stephen prayed, “Lord Jesus, receive my spirit.” Then he fell on his knees and cried out, “Lord, do not hold this sin against them.” When he had said this, he fell asleep.”
When I went to wake her, a stream of blackish blood had dried across her cheek as she slept. Sometimes I would hold up my hand to block the right side of her face from my view, so that I could only see her left, so I could see the girl I recognized, my sweet Allistaire. She would just cry and cry holding her little hand up to her right cheek. She couldn’t close her jaw on that side, her teeth wouldn’t fit together, making eating difficult and painful. Her eye was so bulged out and full of trapped fluid that I could barely see her iris. I gave her as much oxycodone as the doctor allowed and let her sleep except for brief periods of eating. I sat on the bed in the dark, only the glow of the computer screen visible.
Outside the world was bursting with life on beautiful fall days. We were trapped in ever-deepening darkness.
At some point in the span of these brutal days, it suddenly occurred to me, the thought seemingly out of the blue…I am not afraid. I am not afraid of Allistaire dying. I am not afraid of the many awful ways situations in my life may turn out. The realization shocked me but as the words formed in my mind, my deeper self affirmed, fear no longer has me caught by the throat. I am released. I have been freed from its strangling grip.
When I read about the woman, already raped, about to be beheaded, the woman who seemed to smile as she said, “Jesus!”…I nodded my head, yes, yes I can see how such a thing could be true.
People say to me all the time – ALL the time – I don’t know how you do this. Behind such an astonished statement is the desperate hope that we will never be forced to endure such realities. We look at our weak small selves and proclaim – I could NEVER do that! Because we don’t want to, because we have created some sort of system in our mind, some law of the universe we desperately hope is true, that if I can’t endure something, I won’t have to right? But the truth is – the world IS full of suffering and human beings have had to endure terrors far beyond their little girl having cancer and having to watch a tumor gnaw away her face. We are resilient beings. You do what you have to do. We are overcomers and we crave such stories, it is core to our humanity.
With tenacity, with grit, with determination, with perseverance, perhaps with sheer rage, I can make it through this. I can make it through, if even the worst comes to Allistaire. But. This is human effort. This is what my flesh can muster up.
The paradox, the absolute resplendent beauty and otherness of God says, “No. No Jai. I will use these circumstances with Allistaire to tear you limb from limb. I will allow you to be decimated. I will crush you so that you gasp for breath. I will gouge at your heart. You will know anguish and darkness. Panic and terror. And at long last when I have laid you to waste your faint heart will groan and I will incline My ear to you. And beyond all comprehension you will come to know a strength you could not have imagined. You will know a peace that surpasses understanding. You will drink of Me and not grow faint. You will soar on wings like eagles.” These used to be just pretty words. Words I believed, but pretty little words you pat on the head and paint in some scrolly font and frame on the bathroom wall.
How many times have I in desperation, with tears said to Allistaire’s various doctors, “but I don’t know how to let her go. I don’t know how to take her home to die.” As I sat in the darkened room on the very grimmest of any days in this long fight, I felt rest. I am not afraid. Oh, I am radically sad, to my very core, but fear no longer saturates, suffocates. It comes to this, at long last I believe the Lord will actually provide all that I need in the moment – not only to endure but to experience Him turning darkness into light, not because He changes my circumstances, not because He ends my sorrow, but because finally I have tasted of Emmanuel – the truth of “God with me” has sunk yet deeper into my very marrow. I once read a book as a teenager, Abide In Christ, by Andrew Murray. I abide in Christ as Christ abides in me. Sounds so simple yet mystery. I have come to believe – believe – how small a word, how utterly insufficient – nevertheless, I have come to believe that whatever my need, the Lord will meet me in that moment, in that circumstance, and supply in abundance.
Could I endure being publicly raped? Could I say yes to Christ knowing if I denied Him they would stop torturing my child? Could I bow to the blade that would soon decapitate and find joy in that very moment? Can I know peace and even joy in the midst of incomprehensible sorrow should Allistaire draw her last breath? I do not claim to know how the grace will come but I trust that God will be faithful to meet me fully in each moment and supply all I need to keep seeking His face – that even in the very darkest days He can make my face radiant.
It was odd to sense such peace in face of the thought of Allistaire’s death on the very threshold of the coming chemo we hoped would turn things around. In the very span of days that the Lord seemed to remove the last stranglehold of fearing her death, there was hope that there might still be some way through. The peace was unrelated to the hope of chemo working. The peace lay coupled with death, yet, like burrowing through dark soil and rock, while you hope one day to come out into the light , you count as victory any forward motion.
It has been 22 days since Allistaire began chemo for this round and 16 days since her first dose of Mylotarg. Night and day. You can now hardly tell there is anything off with her eye. You have to be looking for it to see it. The bleeding has stopped, her sinuses no longer run, her cheek and eye seem normal in size, her double vision is gone, the pain is completely gone. All that remains is numbness on the side of her nose and upper lip and an occasional expression with her eye that is not completely normal. She is happy and full of joy and giddiness. You would not know she had cancer unless you knew she had cancer.
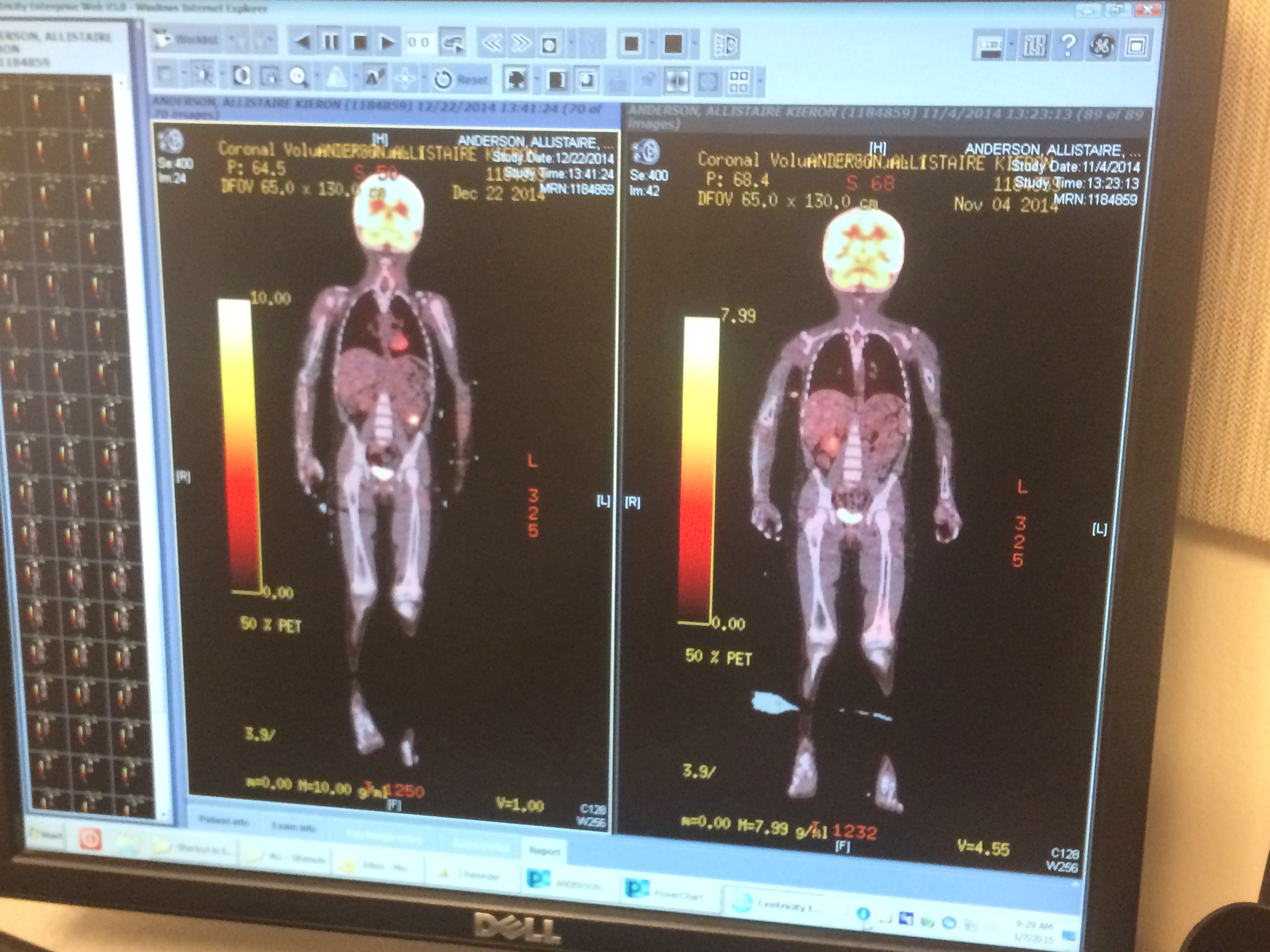
Today I stood in front of two large computer screens with the radiologist, who took considerable time to explain the images and measurements from yesterday’s brain MRI. The actual dimensions of both “granulocytic sarcomas,” or chloromas or tumors, have diminished only somewhat. The larger tumor on the right is at its widest still just over 4cm. The most impressive impact of the chemo is not best understood by measurements in centimeters but the images – wow – the vast majority of the inside of the tumor shows up black on the image – dead cells. There is really only a “thin residual enhancing rim of the cellular tumor.” This is most dramatically seen on the tumor on her right side in the “maxillary sinus,” where it no longer pushes up on the orbit/eye and no longer pushes in on her sinuses. The radiologist informally said it looks like about 80% of the bulk is gone. I won’t lie, it was pretty disturbing seeing the images from the September 29th MRI. Every last bit of space was full of leukemia and it clearly had nowhere to go except into her bones. Thank you God. Thank you Mylotarg.
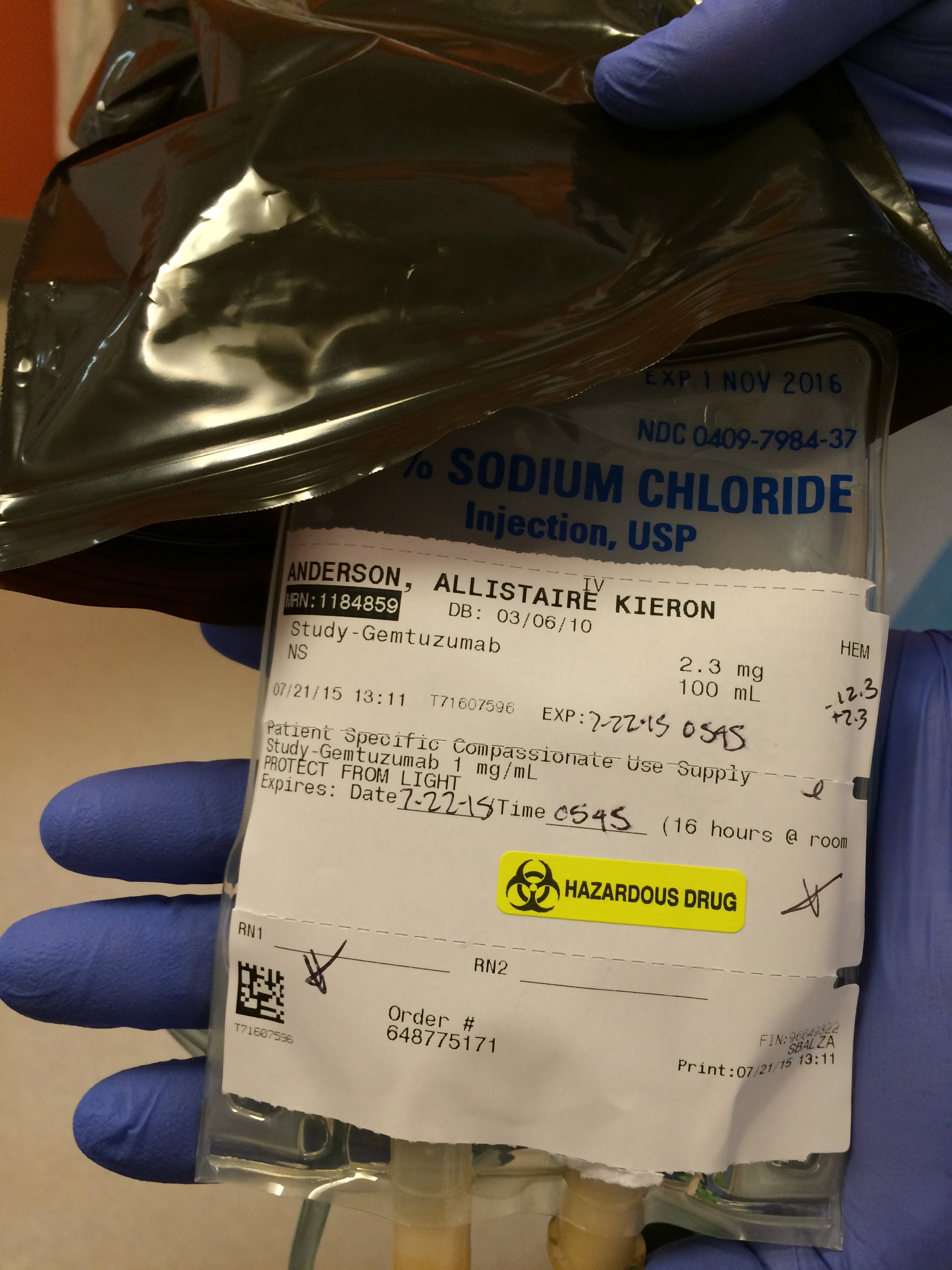
Speaking of Mylotarg, Allistaire and I, along with Solveig who we joyfully had with us over her fall break, had the honor and joy of meeting Dr. Irwin Bernstein. He is both a lead researcher at Fred Hutchinson Cancer Research Center and Chief of the Division of Hematology/Oncology and Bone Marrow Transplant at Seattle Children’s Hospital. This is THE guy who invented Mylotarg – okay, it was his lab that created this monoclonal antibody drug conjugate that targets CD33 and then unleashes the cytotoxic power of calicheamicin on leukemia cells! It was just so incredible getting to sit down with him – this man who for decades has worked on cancer research and whose perseverance, brilliance and team work intersected our lives to literally save Allistaire! I attempted to fully overwhelm him with my gratitude that he and the other folks in his lab would be spurred on! Hopefully seeing Allistaire’s sweet face and a gruesome picture of her face pre-Mylotarg gave him encouragement that what he does has real, tangible impact! Ever wonder why I am such a promoter of Fred Hutch? This is just one example of why. So much of what benefits Allistaire as she is treated at Seattle Children’s comes from the incredible science being done at Fred Hutch!
The other thrilling development is that last week I met with Dr. Cooper, Allistaire’s primary oncologist, Dr. Law, her cardiologist and head of the heart failure and transplant team and Dr. Bleakley, our primary bone marrow transplant doctor. Also present in support were Jeff and Karen on the PAC (Pediatric Advanced Care) team and our social worker, Megan. While I will hold off in explaining the details, in short, the outcome of the meeting was an agreement to aim toward getting Allistaire to transplant as fast as possible. With Allistaire’s ejection fraction on her last echo being 45, she has finally reached the threshold for transplant. There is a lot more to say on this subject but for now, the point is, we are now in a position with Allistaire’s cardiac function to consider transplant! I can hardly believe she has made it this far. Dr. Bleakley proposed a very interesting transplant option that I initially wanted to spit right out of my mouth in rejection – however, after more information and consideration, it seems it may be an incredible option for Allistaire. A number of tests are underway to determine our options moving forward. The most immediate question is what chemo(s) to give Allistaire in the coming, and hopefully last, round of chemo before transplant. While Mylotarg has been extremely successful for Allistaire (at least based on the brain MRI – we still have to see what’s in her marrow in the upcoming biopsy) it has in the past, when given in one large dose, been associated with VOD (Veno Occlusive Disease) during transplant. Dr. Cooper is exploring chemo options available for Allistaire.
A month ago, two months ago, I just felt flat tired, worn down utterly. Allistaire’s great response to Mylotarg along with the possibility of a bone marrow transplant in the relatively near future has created traction and, man, just gives you something to aim for instead of feeling like you’re stuck in an never-ending circle. This week marks one full year since this most recent relapse. We have lived in this wee hotel-like room at Ron Don for one year. Had you told me on October 24th 2014, that I would still be living away from home a whole year later, without having even gotten to transplant yet – well, I could never have imagined how I would get through all that has transpired. The Lord knows what is to come. Hem me in Lord, behind and before.
We just have so much to be thankful for. Thank you to the mom and daughter who gave Allistaire the obnoxiously large Frozen balloon and the purple hippo – just because – because you cared though you never met her. Thank you to Dr. Nixon, the radiologist, who took the time to answer my myriad of questions, thank you to the person who gave me that Trader Joe’s card so I could buy lunch and dinner and dried strawberries that Allistaire likes after her yucky medicines. Thank you to the unknown person who sent me that Kari Jobe CD – I hit “4” over and over and sing out loud in my car, “I lift my eyes, I lift my eyes. Maker of the heavens. Keeper of my heart!!!!” Thank you to my parents who just keep helping to take care of Allistaire and showing me so much love. Thank you dear friends who have provided us with airline credit and tickets so Allistaire and I can go home and Solveig can be here with us and Sten can fly out to see us and miss less work than if he drove. Thank you to my in-laws who help us so much with Solveig. Thank you to my sweet husband who works hard at his job and keeps things up so well at home – including my ridiculous plant collection, far too populated with ferns. Thank you to so many of you who have given financially to cancer research. Thank you, thank you for so many of you who have fallen on your knees before our Lord, who have wept on our behalf.
“Do not look at what you do not have, at what will be loss, rather, be expectant, be on the look out for what I will do, for the bounty I will bring,” the Lord softly declared to me on that gray December morning in 2011. Oh Father. You have been faithful, so faithful. You have become more dear to me than I could have imagined. You have ravaged me and shocked me at your ways. Your words have taken on flesh and color where once they were just dry bones. You, Oh Lord, have been good to me. How I love you. I prayed to you on so many first stars in the night sky, “Father, should one day something happen in my life that threatens to cause me to deny you, to leave you, hold me close, do not let me go.” You have heard my cry. 




























































































































































































{kind=link}
{kind=link}